If it was all about lipids in the blood, Ezetimibe would affect glucose metabolism, but it doesn’t.
Interestingly, ezetimibe (at least in addition to statins) and proprotein convertase subtilisin/kexin type 9 (PCSK9) antibodies do not seem to have an impact on glucose metabolism [9,32,33]. This would indicate, that the increased risk is primarily related to modulating the activity of HMG-CoA-reductase.
@John_Hemming CoA is mentioned here and may be of interest to you.
The clinical significance of the observed increased risk for new onset diabetes with statin therapy is unclear as in most situation benefit of statin induced LDL-C lowering dramatically outweighs the risk of new onset diabetes. Furthermore, statin therapy decreases overall mortality in primary and secondary prevention settings. Nevertheless, it may be prudent to evaluate glucose levels regularly in patients with metabolic syndrome on higher doses of statins.
Why would you listen to anyone in this forum? How many people in here are top expert gerontologists or PhD researchers or doctors?
If you actually listened to what he said, instead of obsessively sneering at his credentials, you’d notice he cites sources for what he says.
It is easy enough to find doctors who admit that their medical school training on diet was terrible. And you can plainly see that any advice they have on diet is useless because they are themselves fat. If their ideas don’t work on them, why would you bother trying to apply it to you?
Cholesterol starts with the availbility of Acetyl-CoA. Some of the Acetyl-CoA gets converted to Cholesterol other parts of it go to the nucleus or for other things.
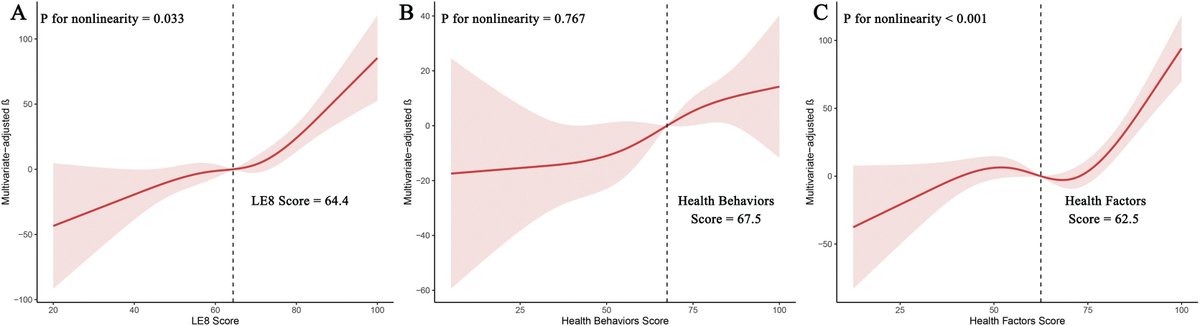
Maintaining ideal cardiovascular health is associated with higher serum anti-aging protein klotho in the middle-aged and older populations
Maintaining ideal cardiovascular health (CVH) is believed to have potential anti-aging benefits. The American Heart Association (AHA) recently updated the “Life’s Essential 8 (LE8)” metrics to measure ideal CVH, but its connection with the anti-aging protein klotho is still unclear. We aimed to explore the relationship between ideal cardiovascular health and serum anti-aging protein klotho in a nationally representative US middle-aged and older population.
Here’s a step-by-step guide to become a LDL cholesterol denialist, which Peter Attia says, paraphrased “is the most dangerous thing I see”.
Go on keto diet.
Lipids increase.
“But keto diet is good!”
That means that lipids increasing being harmful is fake! Because keto double plusgood!
Search for obscure papers from late 90’s using observational studies to get all of the patients with parasitic infections, liver disease, cancer and frailty who get lower cholesterol from it to find lower cholesterol to be harmful.
5.1 Search for any such paper, actually, they can be recent as long as they are observational. Bonus points for less adjustments for confounding factors like parasitic infections!
Ignore strong research methodologies like clinical trials and mendelian randomization that control for these confounding factors.
Find ways to cope with the cholesterol denialism, it could be ‘insulin resistance’ ‘LHMR’, ‘healthy lifestyle’, have to ignore point 6. as otherwise you would know those studies find risk factor independence!
Soothe yourself with stories as you are on the proven wrong side of history (see step 6 and Peter Attia’s point)
Ignore it all when people told you already about this, keep posting about, after all ‘lies that are repeatedly told become the truth’ (" Illusory truth effect")
In the algorithmic hellscape reinforce step 9 over and over so you literally cannot see truth even if it is pointing you right in the face.
Interesting, i had thought the relationship was u shaped between klotho serum levels and diseases of aging.
There’s an interesting vit d link:
" Moreover, Klotho may be involved in the negative regulation of vitamin D by regulating 1α-hydroxylase expression [23]. Klotho−/− mice show a high vitamin D activity and exhibit features of premature aging, which can be reversed by normalizing vitamin D [24], implying the premature-aging-like features might be due to hypervitaminosis D. Conversely, overexpression of Klotho leads to vitamin D deficiency [21], which has also been reported to promote aging"
If the trend in recent years has been to progressively reduce desirable LDLc levels in patients at high and very high cardiovascular risk, some questions arise spontaneously: ‘Having a vast and extremely effective pharmacological therapeutic armamentarium at our disposal, to what extent can we reduce the levels of LDLc safely and what is the optimal LDLc level that can guarantee a further reduction in cardiovascular risk in these patients?’; but above all, can we ask ourselves: ‘So what is LDLc for and why not reduce it—almost—to zero?’.
An ever-increasing amount of scientific evidence is leading clinicians to start lipid-lowering therapies earlier and with more ambitious therapeutic targets; LDLc concentrations at extremely low levels achievable through the use of innovative molecules such as PCSK9i have not only been shown to have no deleterious side effects for health, but indeed, the benefits in terms of protection from CVEs for LDLc concentrations < 20 mg/dL are even more marked and should not scare clinicians nor patients, certainly up to concentrations not exactly equal to zero but at least equal to or higher than 12.5 mg/dL.
So according to what I’ve read, that should increase microbial burden and as LPS goes up you should get T2D. If you have a great gut lining, a great microbiome including oral microbiome then maybe nothing happens. Otherwise I’m guessing the first one to 12.5 wins T2D.
Lol, you mean REAL evidence? It mostly comes from Lustgarten’s book about the microbial burden written, I think, in the late '90s. A great read. I’m not trying to prove anything and don’t want to argue, but I do still think you guys are deleting an important part of your immune system and it won’t lead to longevity.
Clinical trials showing increased diabetes risk from all kinds of statins, bempedoic acid, PCSK9i etc. would be sufficient to prove that lower LDL = higher risk of T2D. But because that is clearly not the case, the hypothesis fails.
but I do still think you guys are deleting an important part of your immune system and it won’t lead to longevity.
My hypothesis is that type 2 diabetes is your body requiring higher levels of blood sugar to combat infections. It’s not the increased blood sugar per se which causes inflammation or rotting of tissue, it’s the infections your body is fighting. So addressing blood sugar via keto etc. is wrong and detrimental to your longevity.
Of course I won’t provide any evidence for my claim and I don’t want to argue (because I know I’m right).
Right. So the invasion by the microbial burden (LPS) is what sends the signal to increase blood sugar and also lipids. I don’t know how increasing blood sugar helps, but I like it, because taking Rapamycin increases blood sugar and lipids. Therefore lowering microbial burden without it really increasing. So rapamycin should reduce microbial burden. But only if you don’t treat the high blood sugar and high lipids. Which by themselves aren’t so bad, they just normally go up with the invasion in order to help.
Don’t worry I do treat my high blood sugar and lipids. It’s just a theory.
I was being sarcastic, but as seen in the ITP, combining rapamycin with acarbose, metformin or the flozins increases lifespan even more than rapamycin by itself, indicating that the increases blood sugar (and cholesterol) on rapamycin is likely detrimental to longevity but that effect is more than outweighed by rapamycin’s beneficial effects.
The exact cause/s behind type 2 diabetes is still unknown and in some statins probably more related to their effect on vitamin K2 and CoQ10 synthesis inhibition than on their cholesterol lowering effect, hence supplementation with both along with using a flozin and/or acarbose will likely compensate for that.