I broke this out from another thread on Lp(a) to allow that topic to stay on subject. I wanted to steer the discussion into prevention and treatment of CVD since it is likely to affect everyone on here sooner or later. For me, I’ve been on Rap for about 5 years (currently every 10 days 7mg with GFJ), but I can’t say its done anything for me as far as my cardiac health goes.
So, I’ve picked up some knowledge on this subject over the last few years, at least as far as it affects my own health. I’m willing to take educated risks for me in how to treat and prevent it, even things I would not suggest others try… I’ve heard several LONG Dayspring interviews multiple times (a series on Attia’s podcast several years ago) and more recently an excellent series with Simon Hill, which I highly recommend anyone who is ‘at risk’ and not on a prevention protocol listen to.
The data is overwhelmingly in favor of prevention, but the benefits don’t come for 10 years. I’m looking to speed that up and there are some treatment options that are potentially effective. For me personally (I have a CAC score presently of 200, I’ve recently started a statin after resisting it for years and I have no side effects. Also I cut 80% of the saturated fat from my varied diet, and I’m trying a few other things. The goal is to eliminate the plaque. I’ve spoken with a few cardiologists and most say it can’t be done, but I’ve found another who says he has reversed it on many patients.
I love the idea of PCSK9 inhibitors but I haven’t yet made the leap yet because I’m waiting for more data. I have heard anecdotes of folks on PCSK9+statins who were able to bring their LDL super low and saw meaningful plaque reduction as a result…I’m hoping we can discuss alternate therapies that show promise (with meaningful data even if its anecdotal.
I’m no doctor…and not a researcher, and I don’t even have a PhD.
But I take from your thread that you believe saturated fats contribute or have contributed to the build-up of plaque. I don’t believe that’s been established, and in fact, might argue for the opposite. Similarly with LDL. I personally do not believe that elevated LDL is the concern that mainstream medicine or long-held/established dogma has had us believe. (Thanks Ancel Keys, not!) I question the desire to drive it lower. Much of the science actually shows folks with elevated LDL live longer.
I also believe statin use and the potential negatives associated with it as it relates to metabolic health/IR, and much more, carry some serious risks, even though you say you don’t have any “side effects.”
Lastly, what kind of exercise are you doing/getting on a regular basis? I understand the feeling that if you could reduce plaque, you’d have a lower risk of CVD. I just wonder if that is even possible. In the end, improving mitochondrial health and function and improving all of the other risk factors associated with CD or CVD, such as oxidative stress from many sources as one example, might be a better path to pursue…
Well there is a difference in what you believe right now and what is true.
The evidence is overwhelming against above neonatal or minimum levels of LDL or more precisely apoB. Established in randomized controlled trials and mendelian randomization (genetic studies), which are able to assess causal relationships. Unlike the “folks with elevated LDL live longer” studies, that only find associations.
What Craig said was completely true, statins are very well tolerated for the vast majority of people.
ASCVD prevention isn’t exciting, it’s not a contrarian take that’s real, it’s just very boring atherogenic lipoprotein concentrations over time which is. The good thing is most cases can be prevented. The bad thing is mainstream science & nutrition was correct. They have access to all the latest and greatest papers, after all. Once you take the red pill (look at the causal evidence), you’ll see all the death and destruction this pro-SFA/LDL meme is leaving in its wake.
Dr Dayspring was the person that recently opened my eyes to the dangers of INDEPENDENT risk factors LDL and ApoB - previously clouded by the health influencers/Doctors that insist that if your inflammation markers and metabolic health markers are fine, you don’t have to concern yourself high lipid numbers. Which is the advice I regrettably followed for over 15 years now. Granted, we have to consider evidence presented by both sides of the isle, both have to be carefully considered. My current opinion is that there is NO DOWNSIDE to try and lower your lipid numbers and mitigate the CVD risks, not waiting to get the definitive proof on either side.
Ironically, Vitamin C (self prescribed) is part of my new protocol. Had played with it in the past but could never get my blood levels higher than they were before I started it. This time I’m using a liposomal/cyclodextrin inclusion product called Cyclo C and also Ester C, which is proven to raise blood levels after 24h. I’ve also read Thomas Levy’s book on Vitamin C and in high enough concentrations, there is some intruiging potential.
@aalyman I also was on the path you are on for years. Used CAC score as a metric to my success…if CAC did not increase more than 15% per year, don’t worry about the LDL. That worked until the last year and a half when it exploded from 80 to 200. Still early though. Ive tried all kinds of diets going back 12 years to reduce LDL, and documented the results on a spreadsheet, and none worked. Not even 3 months of vegan diet which I did during covid. I do believe the association between LDL and events is clear. My doctor also is anti-statin, but the evidence he sent me to ‘prove’ his point was a paper that only tracked a 3.5ish year study period. Its unfortunate. These drugs work over time. I think if you listen to Dayspring and scientists dissect the data, you may reach another conclusion. I generally mistrust pharma as well, but proof is in the pudding.
To his credit, my doctor referred me to a cardiologist he knows named James Roberts who also speaks at conferences: https://www.heartfixer.com/IndexCHC.htm...I had a consultation with him recently and we’ll see how his protocol works. My goal is a zero CAC score in however long that takes. Have a look at this website…disregard the 80’s look. He is VERY sharp and completely knows the science. You will see that he is treating ASCVD and having what seems like excellent results.
Whoever suggested to listen to Attia’s podcast that just came out with the Dutch doc…awesome stuff. So interesting. Thanks for mentioning it.
On researching the subject of arterial stiffness, and found that a drug, AMINOGUANIDINE, mat reverse the pathological cross-linking that sugar initiates: AGE products. Anyone have any thoughts here???
Aminoguanidine can prevent the formation of advanced glycation end products and may even destroy certain cross-links.
What are the benefits associated with Aminoguanidine?
Clinical studies show that aminoguanidine increases collagen density in artery walls, reduces LDL cholesterol, and improves the condition of diabetics as well as kidney function.
In a study at the University of Milan, aminoguanidine improved circulation in atherosclerotic patients to such a degree that their capacity for exercise increased by 50-100%.
Above all, aminoguanidine protects fragile proteins such as those of the skin (collagen and elastin), the eyes, the nerves and the kidneys, from sugar-induced damage.
Aminoguanidine also improves sensitivity to the blood sugar regulating hormone and often lowers blood glucose levels both in healthy individuals as well as in diabetics. In animals, it increases longevity and survival rates.
Why take Aminoguanidine?
Many age-related degenerative diseases, such as vascular, neurological and vision problems, originate from glycation and glycosylation, processes in which glucose molecules bind to proteins, “caramelising” them in such a way as to render them inoperative. Increasingly, scientists consider excess blood sugar to be the second most important ‘metabolic catastrophe’ after oxidation that the aging body faces. It seems that rusting (oxidation) and caramelisation (glycation) combine to transform young, strong bodies into aging, weakened ones.
Aminoguanidine is one of only three identified nutritional substances (the others being carnosine and benfotiamine for these products) which can stop this damage. Each of these substances acts through specific mechanisms and their combined use makes for considerable synergy. The aminoguanidine we offer is the hydrochloride form (HCL) used in clinical studies demonstrating its efficacy. As its half-life in the body is only four hours, it is best to spread the dose evenly over the day.
I have no personal experience of using nattokinase and serrapeptase but I sometimes read that people use it to manage cardiovascular disease and even say that the combination can reduce the size of existing arterial placks. I wonder if there are people here with first hand experience from the use of those substances. They are said to have proteolytic and fibrinolytic properties and supposed to reduce scar tissue, improves tissue healing and fibrin-degrading activity. Like I said, I only know what I have found on the internet but find the approach interesting.
Another option to explore might be, Chelation Therapy for Cardiovascular Disease.
Serrapeptase was prescribed some years ago for my high fibrinogen, an independent CVD risk factor.
Taken daily on an empty stomach it reduced my fibrinogen from dangerous level to normal. When I became complacent and stopped taking it regularly it climbed back into dangerous territory.
Update on fibrinogen as a cardiovascular risk factor - PubMed.
" Now, five prospective studies document the excess incidence of cardiovascular events in persons with elevated fibrinogen levels within the “normal range.” Each standard deviation increase in fibrinogen is associated with a 30% increment of coronary heart disease in men and a 40% increase in women. Fibrinogen should be added to the list of major cardiovascular risk factors."
I do still take it. Serrapeptase isnt cheap, so I’ve been trying to see how little I can get away with. I think 500mg per night might be enough for me, although I was prescribed 1000mg.
Taken every other night @500mg definitely was not enough, as my bloodwork indicated. Next test is in a few months. I always have to make a special request because fibrinogen is not routinely ordered.
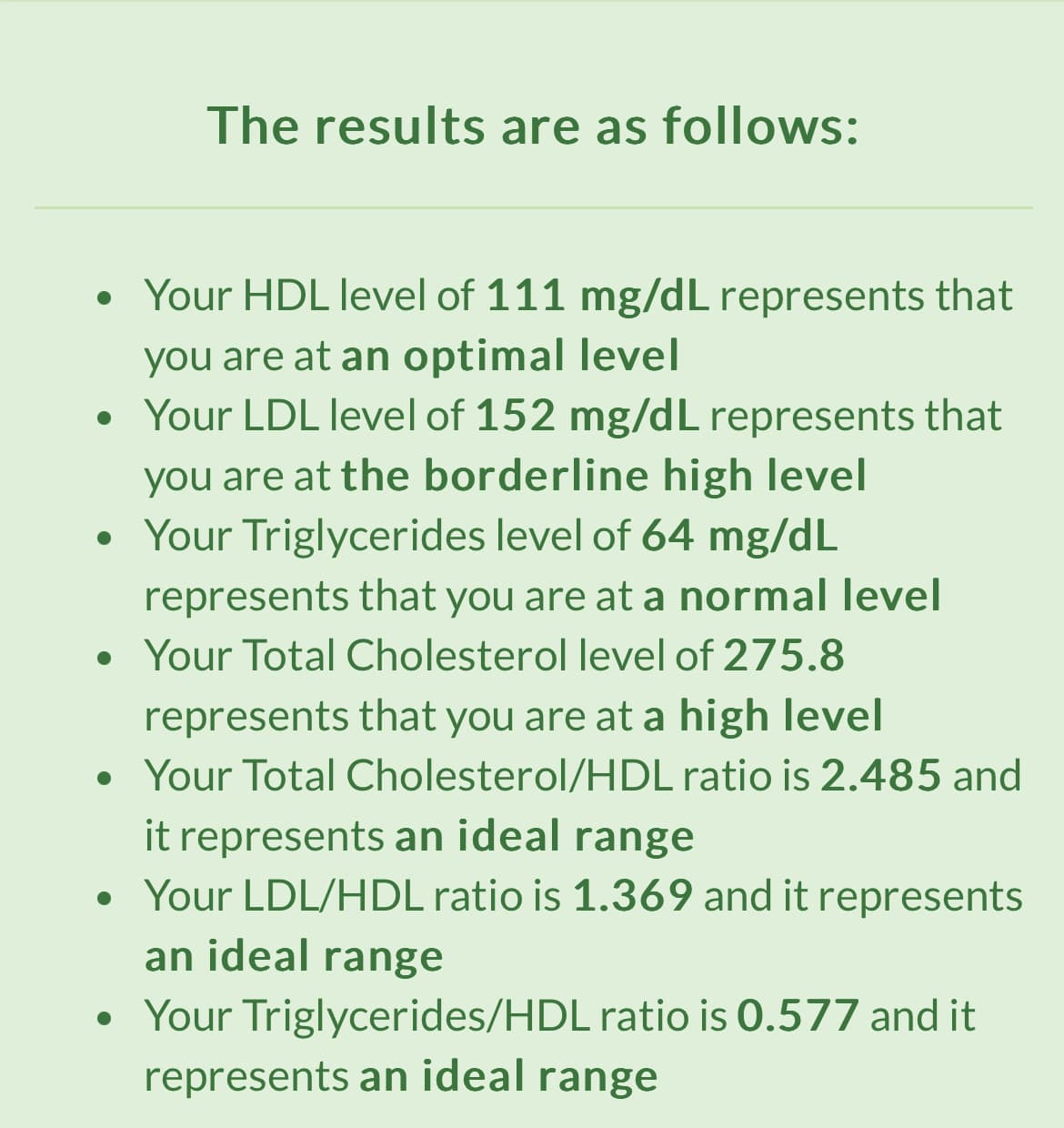
My lipids have been very high for a long time. Rapamycin for 13 years has definitely contributed. Just recently, started taking rosuvastatin, 5mg. After only 2 months, my lipid panel improved much. I check my heart every year (wear monitor for 7 days). Even though my lipids were high, I didn’t develop cv disease. My latest results:
Lara, I wouldn’t be relieved by those numbers at all. HDL is worthless, so all those numbers involving HDL and ratios of HDL don’t mean anything based on all the latest research, other than non-causal associations. I’d refer you the various Attia podcasts with Tom Dayspring as well as the podcast from yesterday. Mendelian randomization studies with HDL show zero effect on CVD. The only number that actually DOES mean anything in there is your LDL, which is quite high if you intend to live a long life without CVD. I’m surprised it’s still 150 despite the rosuvastatin.
I don’t agree w/Attia on everything, but I think he’s absolutely right when he cuts through all the noise and focuses on ApoB and Lp(a).
Hi @LaraPo . The numbers are certainly high. The Rosuvastatin dose you are taking is very low. FYI, they started me on 10mg with the understanding I would go to 20 subject to side effects (none) and a check to see where we are after stabilizing on 10mg. Point is, if you’ve had those numbers for a long time, you may want to be a little more aggressive if your aim is longevity. I’ve been on Rap for 5 years with no meaningful change in lipid levels from it.
I’m not relieved at all. The result just shows a good progress for only 60 days and on a lowest possible dose of 5 mg, which I take every other day. Today the number is 150 but 2 mo ago it was 194. It goes in the right direction. I cannot take a higher dose bc of side effects (skin rash, shingles outbreak, dermatitis, etc.). I’m sure that in couple more months it will be all normal.
My high cholesterol could be genetic - at least that’s what my cardiologist thinks. I do not have CV disease, confirmed by many scans, USs, etc. I even had angiogram done which showed clean arteries. Rapamycin also contributes. I’m not a fan of a statin, and tried it many times in the past unsuccessfully bc of side effects. This time, I go slow with a very low dose. Will report the results in couple more months.
Did you get a coronary calcium scan? If you want to get LDL even lower with minimal risk of side effects, might want to consider ezetimibe (and/or various supplements such as amla, citrus bergamot, psyllium, etc).
Have you tried stopping the Rapa to see what it does to your lipid panel? Otherwise, looks like the statin is helping. Definitely check the apo B, LP (a).
Bizgoz, hope you’re taking everything here with a grain of salt. Ideas to investigate but not just accept as gospel. Some posts above are great, others not so much. Keep up with the statin.