Bigoz, have you looked into K2 supplementation and its effect on plaque?
Effects of vitamins K2 and D3 supplementation in patients with severe coronary artery calcification: a study protocol for a randomized controlled trial.
I have no idea if k2 helps remove plaque. Further, there is soft plaque and hardened calcified plaque and from a MI point of view the soft plaque seems more dangerous.
I wish that I had a CAC score from a decade ago, but then, I wish I had one right now, I’ll have to look into getting one.
Keeping plaque from developing w/in arteries in the first place and attempts to remove or stabilize it are two very different things.
Still, I take Rosuvastatin and have for more than a decade. From https://health.clevelandclinic.org/can-statins-actually-reverse-plaque-buildup:
Q: Can statins actually reverse plaque buildup?
A: Yes. There have been several clinical studies — many of them done here at Cleveland Clinic — that show statins can reverse plaque buildup.
Two statins in particular, atorvastatin, which is sold under the brand name Lipitor, and rosuvastatin, which is sold under the brand name Crestor, are the strongest statins.
Clinical studies using ultrasound in the coronary arteries have shown that when you are on high doses of these medicines, even if you have plaque buildup already, you can stabilize the plaque on statin therapy.
If your LDL cholesterol is lowered below 70 mg/dL, you can even see a regression in the plaque by up to 24%. So having really a low LDL cholesterol level can help stabilize any plaque buildup you have, and prevent further plaque progression.
— Cardiologist Steven Nissen, MD
I used to have access to a CholestTek and chose Rosuvastatin and asked my doc to prescribe 20mg and w/ his permission to “play with dosage.” I started at 2.5mg, then 5, then 7.5 and so on. The response was classical and I settled on 6.7mg (1/3 of a 20mg tablet) though lately being on keto I’ve dropped to 5mg, my numbers are currently LDL 83, a bit higher than a usual ~43 due to being on keto/omad.
I’m a USDOL field nurse (RN) and I oversee care for about 40 injured federal workers at a time, about 200 a year (they come and go). In many cases injured workers w/ ruptured or torn tendons (a very common injury) I often see pretty high-dose statins. Often I find myself wondering, was it the accident that caused the rupture/tear, or was it the statin?
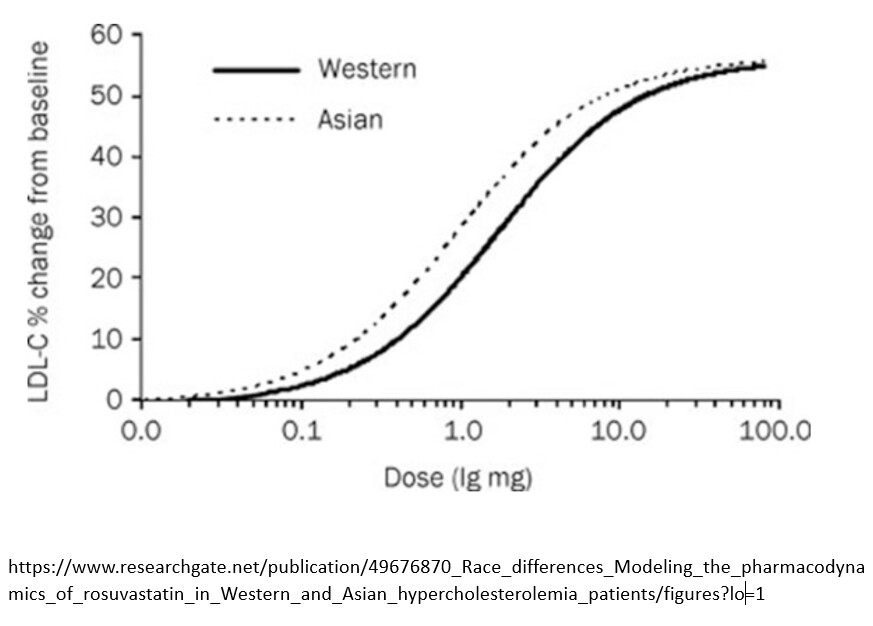
I do wonder if statins are in fact a “wonder drug,” but one that is often prescribed at levels far higher than is necessary. Were I a Practitioner I’d start a patient on a low or very-low dose, test a few months later, then move higher. The pharmacodynamic curve is quite straight, so then choose the dose to obtain necessary changes but not to overshoot, risking adverse effects.