Wait, rapamycin blocks neurogenesis? That seems like a bad thing…
Then I came across this 2022 study by Shi et al. that found that, in knockout mice, “Inhibition of mTOR pathway with rapamycin, a well-established immunosuppressant, downregulated Trem2 in microglia and reduced Aβ plaque clearance indicating that mTOR inactivation may be detrimental in Aβ-associated AD patients.”
It can’t tell whether the rapamycin treatment in this study was started before or after AD was already established. (I understand that rapamycin is unlikely to prevent or reverse AD once it’s established, which is why I’m taking it in my 50s.) Rapamycin admin was apparently chronic (not pulsed) at 2.24 mg/kg/day.
This finding seems concerning. I don’t see any threads on this topic in this forum or elsewhere online. Am I missing something? Perhaps this finding could be explained by the dosage and/or chronic administration.
From Shi et al (2022):
SIGNIFICANCE STATEMENT Mechanistic target of rapamycin (mTOR) signaling pathway is a key regulator for major cellular metabolic processes. However, the link between mTOR signaling and Alzheimer’s disease (AD) is not well understood. In this study, we provide compelling in vivo evidence that mTOR activation in microglia would benefit β-Amyloid (Aβ)-related AD pathologies, as it upregulates Trem2, a key receptor for Aβ plaque uptake. Inhibition of mTOR pathway with rapamycin, a well-established immunosuppressant, downregulated Trem2 in microglia and reduced Aβ plaque clearance indicating that mTOR inactivation may be detrimental in Aβ-associated AD patients. This finding will have a significant public health impact and benefit, regarding the usage of rapamycin in AD patients, which we believe will aggravate the Aβ-related AD pathologies.
Reducing Tacrolimus Levels to Improve Cognitive Function in Kidney Transplant Recipients 2024: “Calcineurin inhibitors (e.g., cyclosporin, tacrolimus) cause endothelial dysfunction and are inherent vasoconstrictors. ESKD patients present an increase in cerebral blood flow, which occurs probably because of inflammation, vascular disease, and disruption of cerebral autoregulation. Nevertheless, cerebral blood flow decreases after kidney transplantation to values lower than those observed in healthy people. Decreased cerebral blood flow is associated with cognitive impairment. Although uncertain, it is possible that calcineurin inhibitors–induced vasoconstriction contributes to this phenomenon.”
I don’t think the article you cited below suggests the effect is unknown, but rather that it is beneficial only before AD onset, as my initial post stated.
There’s no certainty, but as you’ve suggested, the evidence points toward benefit before AD onset–particularly for APOE4 types.
I am trying to understand the contrasting findings from Shi et al (2022). It could be explained by the dosage or administration. I can’t find any other studies addressing Trem2 and AD risk, and I would like to know whether others have seen research on rapamycin’s action on the Trem2 pathway and AB deposition.
This discussion might be an indication for some of us, to use lower doses, This to avoid that too much rapamycin penetrates the blood brain barrier. and letting the system clear the rapa for a few days before next dose.
I can not say we have evidence, but in one part of the lecture given by Prof David Dodick (starting at 28 minutes and ends at he 40 min mark) he speaks of GLPs, metformin and rapamycin in relation to brain health and Alzheimers. This is a reasoning from his point of view and that rapamycin might have a negative effect on Alzheimer’s. But it depends on the timing of the intervention. And one has to consider that he, as a doctor, most likely plays a risk-aversive role. (above all, do no harm)
As I see it, there is a risk, and we don’t have evidence. So what I consider is more of a risk management strategy.
Thanks for sharing the info about these clinical trials, adssx. Do you have a link to the pre-print publication of the CARPE-DIEM results? I see the clinical trial data online but not the study results.
Although β-amyloid plaques probably do not cause AD, it seems unlikely that they’re “irrelevant.”
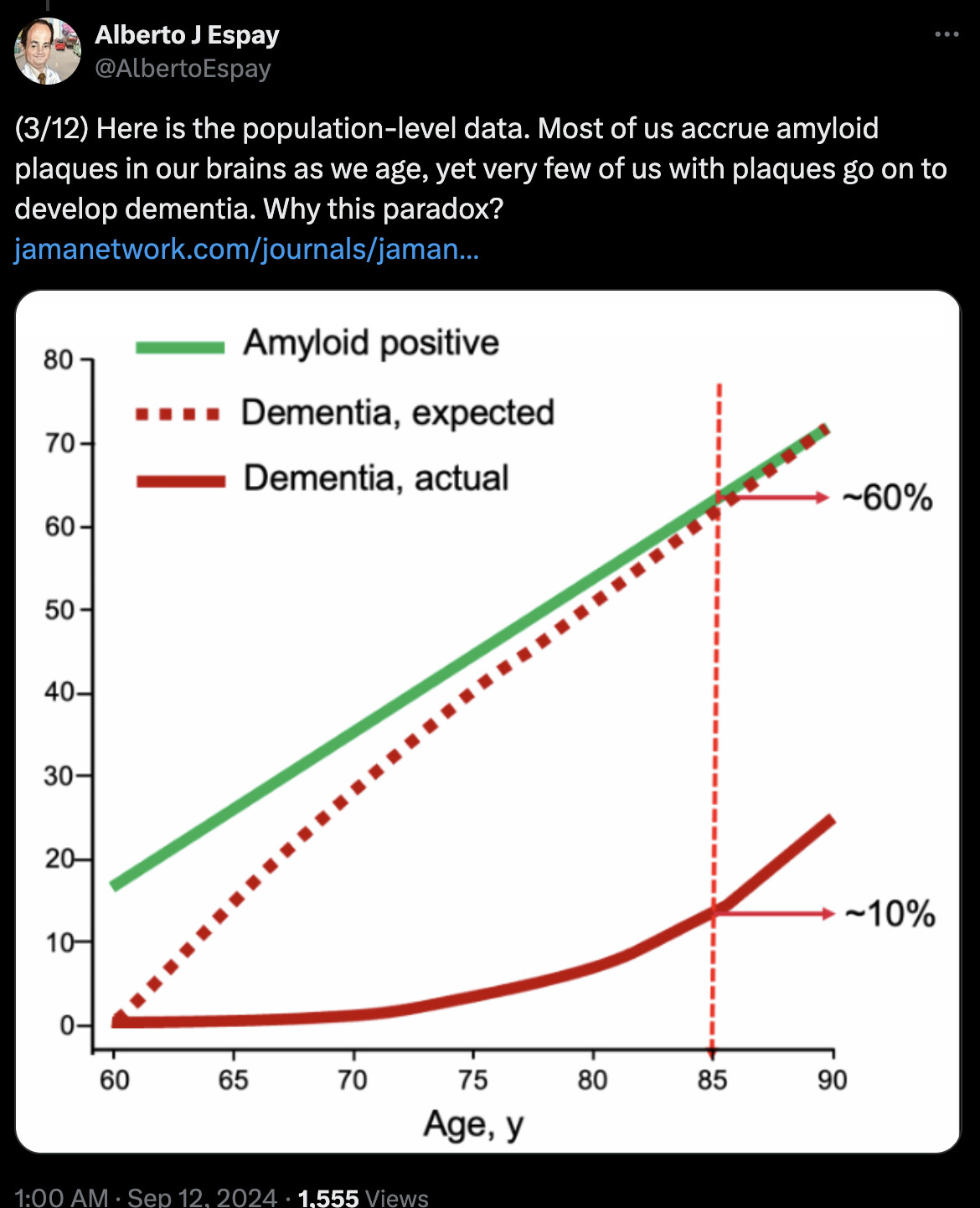
Trem2 activity in the microglia may hold one possible answer to Alberto Espay’s question, Why do most old people with β-amyloid plaques not get AD?
“Mutations in TREM2 were found to disrupt microglial energy state and function, thus sabotaging microglia’s ability to protect the brain against toxic amyloid plaques (Hong and Stevens, 2017; Ulland et al., 2017). Ulland et al. (2017) also found that microglia in AD patients carrying TREM2 risk variants and in TREM2-deficient mice with AD-like pathology were defective in rapamycin (mTOR) signaling, which affects ATP levels and biosynthetic pathways.” (my emphasis)
As I stated in my initial post, a 2022 study by Shi et al. found that, in knockout mice, “Inhibition of mTOR pathway with rapamycin, a well-established immunosuppressant, downregulated Trem2 in microglia and reduced Aβ plaque clearance indicating that mTOR inactivation may be detrimental in Aβ-associated AD patients.”
It seems that the AD pathology has something to do with the brain’s clearance of toxic β-amyloid plaques–that is, it has something to do with autophagy.
The research on TREM2 is new to me, and the Shi et al. 2022 study seems to suggest that rapamycin may downregulate TREM2 and block its potential benefits. That’s what I’m curious about.
I hope someone who read the Shi et al. (2022) and/or knows something about TREM2 and microglial function will respond to this thread.
Thanks, that’s very interesting…and a little unexpected.
I think the thing to remember for both of these is that we are cycling or pulsing rapamycin and mTor inhibition. So I would allow a good interval after taking rapamycin before I would experiment with psychedelics, but the “Psychoplastogens” concept I find fascinating and am reading up on. The mouse study used rapamycin continuously and it took a month before they saw changes. That’s quite different than taking very moderate doses once a week, or less. I think it’s clear that you need mTOR activation, the problem is when it’s over active. Low dose pulsed rapamycin is meant to modulate it, not eliminate it.
That’s my understanding, too. Thanks for affirming my attempt at understanding of the factors at play: high vs. low dosage and chronic vs. pulsed administration.
The other factor seems to be AD stage. It seems that early administration of rapamycin (before cognitive symptoms appear) promotes beneficial autophagy, but late administration (when AD is already established) exacerbates existing dysfunction of the lysosomal system.
This 2023 summary of recent research cites Shi et al (2022) to come to that same conclusion:
"Rapamycin was found to increase the number of autophagosomes and autophagic lysosomes … Rapamycin has an autophagy-promoting effect on Aβ-depositing cells and attenuates further cellular damage by Aβ, which may be one of the mechanisms by which rapamycin can be used to treat patients who have already developed pathologic features. However, the lysosomal system in the brain is less expressed and slower in the later stages of AD and with aging. Rapamycin inhibits mTOR and activates autophagy to clear Aβ. Decreased lysosomal clearance leads to autophagosomes accumulation, causing autophagic stress and promoting the amyloid plaques formation. Thus rapamycin has a complex, even harmful effect on late AD.
[. . .] Furthermore, rapamycin inhibits microglia activation in the brain and reduces microglia proliferation, yet microglia activation may play a dual role in the AD pathogenesis. "
Si-Jia Hou, Sheng-Xiao Zhang, Yang Li & Sui-Yi Xu, “Rapamycin Responds to Alzheimer’s Disease: A
Potential Translational Therapy” (2023) Clinical Interventions in Aging
(https://www.tandfonline.com/doi/pdf/10.2147/cia.s429440)
On that last point, Hou et al cite the following article that elaborates on the “dual role” of microglia in AD: “Microglia are perpetually engaged in a mutual interaction with the surrounding environment in CNS; thus, diverse microglial reactions at different disease stages may open new avenues for therapeutic intervention and modification of inflammatory activities.” Sarlus H, Heneka MT. Microglia in Alzheimer’s disease. J Clin Invest. 2017;127(9):3240–3249. doi:10.1172/JCI90606
This point backs up Carosi and Sargeant’s metaphor of rapamycin as “double-edged sword,” mentioned earlier in this thread by adssx: “Treatment with rapamycin at a later point would carry a higher chance of exacerbating existing lysosomal problems.” (https://www.tandfonline.com/doi/pdf/10.1080/15548627.2019.1615823)
PS, I came to the same conclusion on this point also: To avoid inhibiting neurogenesis, “I would allow a good interval after taking rapamycin before I would experiment with psychedelics.”