I read through an old (and very thorough) thread here awhile ago about metformin … and decided maybe not to take it since it can impair exercise….
However…. It’s in the news again…. Im thinking of taking it… but maybe not every day…. Def not on my weightlifting days…. But maybe on my non workout days and on the day I take rapa….
Currently taking 6mg rapa once per week…
Anyone try this with metformin? Like once a week doses or a couple times per week? Also, if so, what dosage…. Im wondering if low dose (500 mg) of metformin can have some positive impact?
Yes, I have been doing just what you’re talking about. I take it for a couple days after Rapa to tamp down my fasting glucose. I try not to use it if it’s a workout day, but it doesn’t hurt my strength that much.
I have been using metformin for decades experimenting with various dosages and also cycling on and off for extended periods. IMO the effect of metformin on exercise and muscle gain is highly overrated. The effect is subtle at best.
The effect IMO would be like doing 10 reps without metformin or 12 reps with metformin to achieve the same outcome.
My opinion, based on everything I’ve read- if you are not diabetic or pre-diabetic, do not take Metformin. There is no reliable evidence yet that it is of value, or that benefits outweigh risk. Others here will disagree.
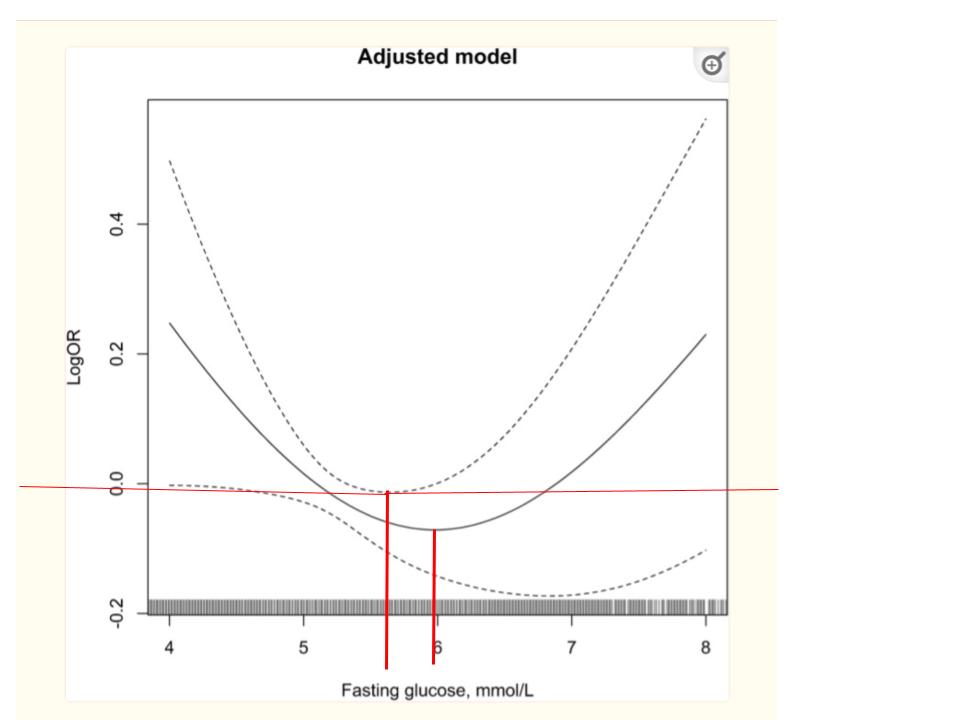
Fasting glucose levels generally increase with age. I choose to take whatever it takes to remain at the bottom of the U-shaped curve.
You also have to consider that taking rapamycin increases fasting glucose levels, so we might need a little help in the form of metformin, etc.
“The overall evidence suggests a J-shaped association between fasting glucose levels and all-cause mortality in nondiabetic populations. Both high and low fasting glucose levels, compared to normal fasting glucose, are associated with increased mortality risk”
"J-Shaped Association
Several studies have found a J-shaped association between fasting glucose levels and all-cause mortality, with the lowest risk at around
80-100mg/dL."
“In non-diabetic patients with ACI, elevated baseline FPG is an independent risk factor for 1-year all-cause mortality, and the two are positively and non-linearly associated.”
My current fasting glucose is near ideal. I do this with metformin, etc.