I followed her she was incredible- genetic factors play a big roll in early age cancer and heart disease. I had my genetics ![]() done from 3 different companies they were all similar. “Dirty Genes” is a great read! I have a couple now that I know I watch and test for specific changes via blood markers.
done from 3 different companies they were all similar. “Dirty Genes” is a great read! I have a couple now that I know I watch and test for specific changes via blood markers.
5 Likes
@agingdoc I couldn’t agree more about the need to find a safe but bold middle ground in our individual pursuit of long health. I find it too easy (a slippery slope) to add one more chemical, and then another as I find more and more “positive results” in scientific studies. Ive been chasing an answer to this personal problem publicly (on this forum).
My concerns include:
- polypharmacy—too many chemicals mixed together that haven’t been tested in combination. Affecting absorption of other nutrients, more side effects, etc
- The “crutch effect”—takes away the motivation to address root causes in lifestyle factors.
My solution (I just started) is an arbitrary one that pushes me in the right direction
- only add one thing at a time to measure effect
- limit non food chemicals that I take regularly to 10 items. If I want to add something, I have to drop something
- take regular breaks from chemicals added to diet (I use zero supplements and medications on my rapa day 0 & -1)
- only buy from high quality sources to make sure I’m getting what I want and nothing I don’t want. This is affordable now that I limit my count.
- focus on lifestyle solutions: sleep, physical activity, sunshine, fresh air, clean water, low body fat, gut health, happiness.
What am I missing?
8 Likes
6 Likes
Wow!
Blagosklonny is brilliant. His concept of regression of cancer cells… and progression of resistant cancer cells simultaneously. Hence, mono-treatment with initial success… ultimately will fail in many cases. If true - changes are needed on how we should treat cancers.
I wish this had more on rapamycin, I see it is coming… although I think Dr. B. is wrong on users should do the highest dose of rapamycin without side effects. Still want to see his rational.
In medication, too high of a dose can be poison. I think rapamycin is no different. Personal experience… my N=1.
6 Likes
“although I think Dr. B. is wrong on users should do the highest dose of rapamycin without side effects. Still want to see his rational.”
This is how I understand that rational. Side effects show that the dose is poisonous and it harms. The dose before side effects start is a normal healthy dose. That “highest dose before side effects” is in fact a low rapamycin dose. When that healthy dose is exceeded the problems start.
9 Likes
Yes… but as Matt Kaeberlein shared with me… what if…
“I understand Misha’s rationale for pushing it as high as possible until you get to side effects. My concern there is that you might be getting to side effects and not know it right away or at all (silent pathology) until it’s too late to reverse the damage. I have no evidence for that, but it’s a concern I have.”
Silent pathology… kind of what Misha was saying about cancer… as you treat one area… a new resistive area starts… undetected… until too late…
10 Likes
After all our best shot to avoid cancer is fasting?
I lost my parents to this disease. I would do anything not to have it.
8 Likes
@Agetron ”your evidence” of damage from higher rapa dosing is your epigenetic test results I assume? Is that enough to draw a conclusion? Do you have any other results (feeling, physical performance, bloodwork) suggesting that your previously high rapa doses were damaging?
I’m just trying to understand this question. Thanks.
5 Likes
Cancer also seems to love blood sugar and cholesterol.
5 Likes
Hey Joseph…
As stated, it is my N=1.
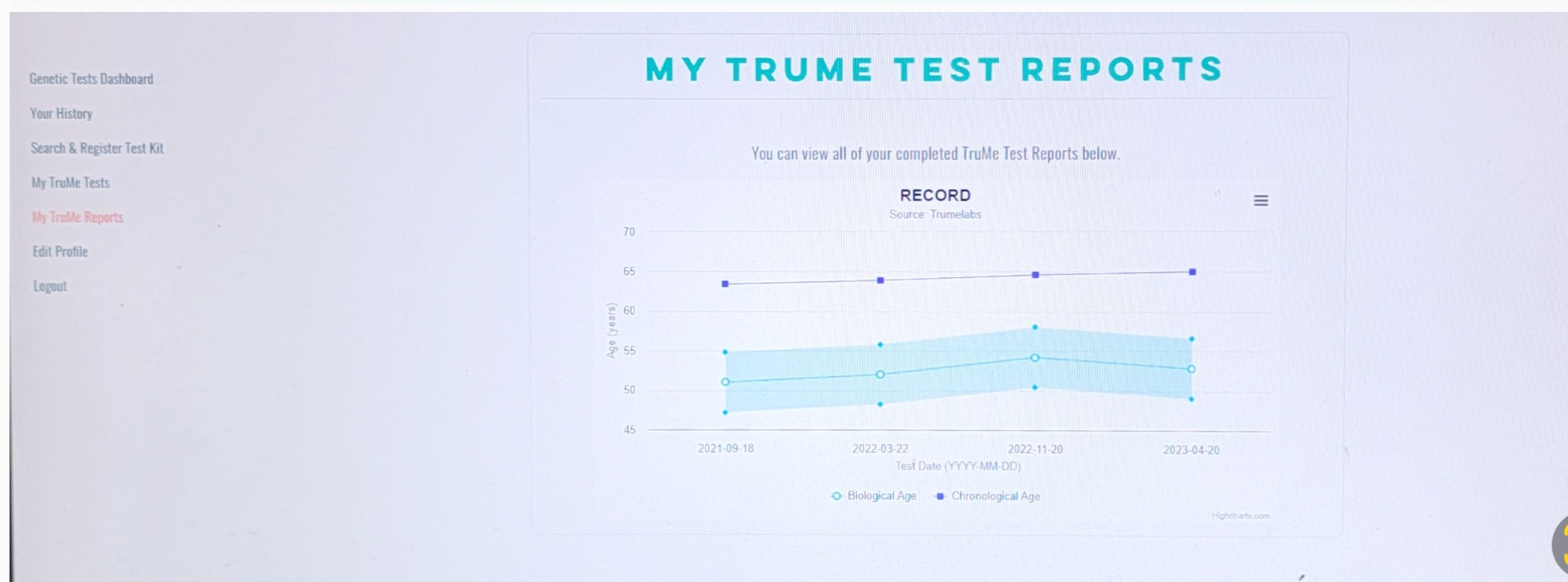
Low dose rapamycin weekly 6-8 mg and after a year of dosing decided to take two biological age markers tests… TruMe used spit for epigenetic methylation analysis.
GlycanAge used blood sample for glycans on proteins… inflammation test.
Two different types of biolgical tests measuring two different hall mark . My results were so significantly off the norm in biological age… that I was queried by the company’s CEOs. Explaining I was on rapamycin seemed a plausible explanation.
Re-took test with similar results.
At two years use of rapamycin, I significantly upped my rapamycin to 38 + every 7-10 days. Thinking all was fine, retested after 7 months of this dosing program. Was shocked to see a parallel rise in my biological aging on both tests.
Immediately went back to 6 - 8 mg of rapamycin weekly and at 4 months both test (TruMe and GlycanAge) showed a big drop to a younger biological age. Retested at 4 more months and was back to the before high dosing numbers. Matt Kaeberlein also sresses the dose could be detrimental and unnoticed.
I never notced anything in my 7 months of higher dose but slight swelling of ankles and face.
Matt Kaeberlein and Peter Attia take no more then 8 mg weekly with breaks. They should have the best perspective on dise. Certainly not doing more.

13 Likes
@Agetron Thanks. That is powerful N=1 evidence of Rapa dosing being too high to risk continuing. The swelling symptom is interesting. I have had a bit of ankle swelling occasionally since taking Rapa. I wonder what that is? My kidney biomarkers are good. My sodium is good. Heart function? Did your swelling disappear?
3 Likes
Yes, the swelling disappeared when I reduced my dosage to 6 to 8 mg.
I initially thought the swelling of my ankles was due to taking minoxidil, which was said to have that side effect. But, I’ve continued to take minoxidil and still don’t have any swelling, so it seems it was the high rapamycin dose.
Added those TruMe and GlycanAge charts to the post above.
3 Likes
Thanks that is great info. How are you currently taking your rapamycin, with/without grapefruit, olive oil, etc?
4 Likes
Cholesterol? ![]()
![]()
I thought “high” cholesterol was related to longevity accordingly with the lasts studies.
1 Like
Lowering cholesterol via statins or diet has proven repeatedly to lower incidence of heart attacks, strokes and even all-cause mortality in clinical trials.
What you’re refering to are observational trials where a U-curve can indeed be seen with cholesterol levels. The reason for that is not that low cholesterol is bad for you but that people with cancer have low cholesterol due to the cancer cells “eating up” your cholesterol and sugar.
Low Cholesterol, Greater Death (youtube.com)
Cancer cells require cholesterol for rapid proliferation and tend to accumulate a high amount of cholesterol for which they either rely on up-regulated cholesterol biosynthesis or by enhancing uptake of cholesterol. Many of the cancer cells lack a feedback mechanism for controlling cholesterol uptake through LDLR expression as compared to normal cells/ tissue
Influence of cholesterol on cancer progression and therapy - PMC (nih.gov)
5 Likes
Hey Charles - for many months now… I take a fresh squeezed red grapefruit (about 5 fl. Ounces) and a 2 mg pill of rapa.
Currently, on Zydus. I’ll do a Labcorp test of GFJ and 2mg rapamycin/zydus next week and share the results. I am assuming to hit 6 to 8 ng/mL. We will see.
2 Likes
Thanks for the feedback.
I’m new to this world, always good to learn.
My cholesterol has always been well below, I was happy with the increase in the last few months after starting/increasing my EVOO consumption.
2 Likes
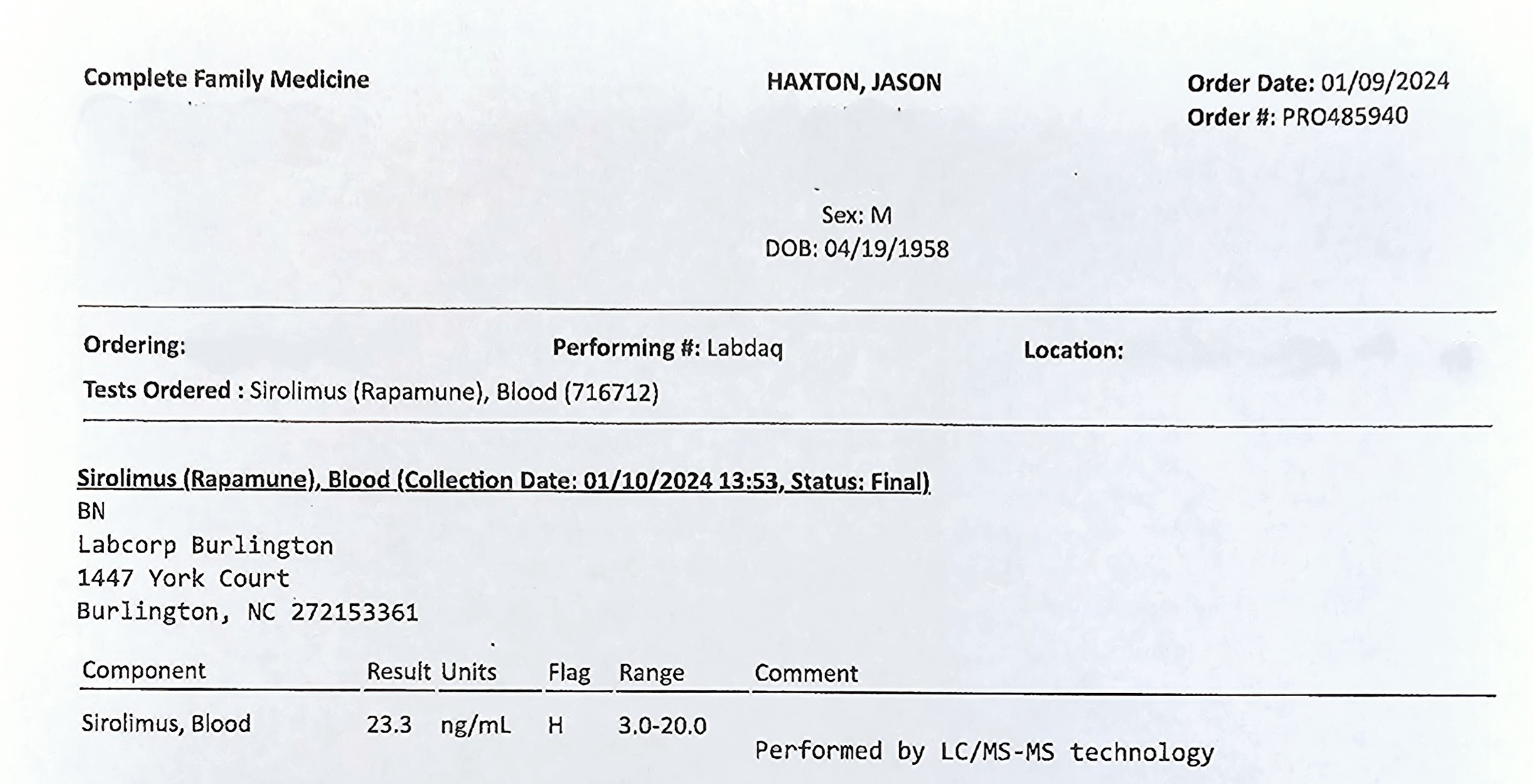
I took two of my 2 mg zydus pills (4 mg total) with the juice of one fresh Red Grapefruit. Blood test at 2 hours post dose.
My trough was zero… hadn’t had any rapamycin for 2 weeks.
Results were 23.3 ng/mL.
Almost 6 times multiplication of dose with GFJ.
6 Likes
The optimum range is 5 - 20, as you see in the table, and yours is 23. However the expected range is a measurement taken 24 hours after the dose. So your number, as I understand it, doesn’t provide any meaningful information. How do you interpret your number? Is it good or bad? Does it have to be lower or higher 2 h after you take rapamycin? Nobody knows. I see a problem in that. Any thoughts?
I think you need to test it 24 h after the dose, as required, to see what’s actually in your blood. Then you’ll get a correct trough level, which will show a degree of your immunosuppression (between 5 and 20).
Hmmm… I beg to differ, the importance for me is the initial blast c-max or t-max both are fairly similar. I have taken about a dozen labcorp readings. Trough and c-max.
Then through half lives it is eventually out of your system (or at least below 1ng/mL) which is my interest. What is happening 24-hours later is the slow dissipation of the rapamycin from your body.
Seeing 23.3 at 2 hours post dose sets off alarms as I had a negative biological impact when I was getting in those higher numbers (c-max 38 ng/mL for 7 months).
For now, I can live with a 12 ng/mL c-max - I don’t want any higher. I will see what the impact is after 6 months on my TruMe and GlycanAge tests. Maybe we are looking for different things. From my experience, I tend to agree with Matt Kaeberlein on high dosing: “I understand the rationale for pushing it as high as possible until you get to side effects. My concern there is that you might be getting to side effects and not know it right away or at all (silent pathology) until it’s too late to reverse the damage. I have no evidence for that, but it’s a concern I have.”
I do have evidence of damage based on over a year of monitoring the higher dose two different biological markers tests and lowering the dose to get a reversal.
7 Likes