After listening to the latest talk from Dr. Kaeberlein and reading the works of Bruce Ames (95 yo Biochemistry Professor UC Berkeley), the one thing that stuck out was that he said to cure your deficiencies first for healthspan and longevity. After that, exercise, sleep, diet, and socialization are important. Finally supplements.
So, I thought we should create a thread to list things that most/many people are deficient in and ways to treat it as this is the first step towards longer lifespan\healthspan and we often overlook it. I’m going to start off with the two biggest deficiencies I know of:
1. Omega-3s - 70% of American adults and 95% of children do not get enough Omega-3s.
Low EPA and DHA levels in red blood cells were found to be associated with increased all-cause mortality in a study of 6,501 elderly women followed for 14.9 y (32). A metaanalysis reported that each 1% increase in plasma DHA/EPA was linked with a 20% decreased risk in all-cause mortality (33).
Low blood levels of DHA/EPA were shown in a 5-y study to be associated with a faster rate of telomere shortening, a marker of cell aging (36). Supplemental fish oil (2.5 g/d) slowed telomere shortening and lowered biomarkers of oxidation in older adults (37). Daily supplemental DHA (2 g/d) increased the rate of clearance of amyloid plaques in people with mild cognitive impairment (38). DHA/EPA are important for vitamin D steroid hormone effectiveness (13). Evidence of their role in reducing the risk of heart disease has been obtained (39, 40).
Solution: 1 - 2 g of Omega 3 supplementation (2X EPA vs DHA) - or eat a lot of fish/fish oil.
2. Vitamin D3 - 70% of Americans are deficient as are 50% of American children
Vitamin D levels are inadequate in 70% of the United States population. Almost all dark-skinned people residing in northern latitudes are particularly deficient (12, 13).
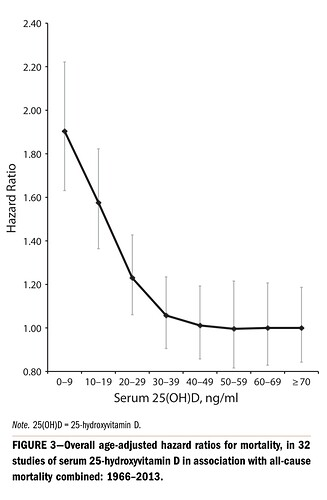
Extensive evidence shows that vitamin D deficiency causes—or has been associated with—a large number of diseases that affect healthy aging, such as all-cause mortality, cancer, cardiovascular disease (CVD), diabetes, brain function, and so forth. Considering this high level of deficiency and the important implications of vitamin D interactions, it is particularly important to tune up metabolism (15) with respect to vitamin D. See SI Appendix, SI-3 Survival V/M That Are also Longevity V/M for the large literature on vitamin D clinical trials and Mendelian randomization studies.
Here you see the Hazard Ratio for low D3. You need at least 30 Serum ng/ml, but preferably 40.
Solution: 1,000 - 10,000 ius of Vitamin D3 supplementation (25 mcg - 250 mcg). I took 5,000 IUs daily, but was still deficient. I now take 10,000 ius. You also need to take Magnesium to absorb D3 and vitamin K2 also helps. I take 2 g of Magnesium Citrate daily and a MK7 K2 supplement on Mon-Wed-Fri as K2 has a long half-life.
Note: Alzheimers and Dementia patients as well as those at risk of both should avoid supplementing with vitamin D. https://onlinelibrary.wiley.com/doi/full/10.1111/acel.13670?campaign=wolearlyview#.YtR9Mq-l2Sk.twitter
3. Magnesium - 45% of Americans are deficient
Mg is present in the center of the chlorophyll molecule, with plants being a major dietary source, together with whole grains, nuts, and seeds (41). Mg deficiency affects about 45% of the United States population and has been associated with increased all-cause mortality, poor DNA repair capacity, increased risk of lung cancer and various other kinds of cancer, heart disease, telomere shortening, and risk of stroke (SI Appendix, SI-3 Survival V/M That Are also Longevity V/M).
A recent review on the subclinical effects of Mg deficiency makes the case that this deficiency is a principal driver of CVD, a worldwide underrecognized problem, and thus that it is a major public health crisis (42). Mg is required to convert vitamin D to its active steroid hormone form (43).
These are just 3 of the most common deficiencies. Can anyone add any that affect 40% or more of the population?
It should be easy as the typical American diet is really deficient in so many areas. ![]()