The main thing for me is that my highest levels coincided with when initially went from half to full dose of Repatha (which generally is expected to lower Lp(a) by 15-40%…)
The other think I can think about is that I sometimes end up eating more nuts than I perhaps should, but I don’t have the exact timing of that.
I did have to change from Praluent back to Repatha starting a little over a year ago, so I wondered if Repatha isn’t as potent in lowering Lp(a) as Praluent. Still wondering if empagliflozin is involved at all.
Well it seems like this Lp(a) thing may not be totally settled. So, I might revise my test Lp(a) one time only, and go with a really low Lp(a), no need to retest. A really high Lp(a) no need to retest - at least until we have good drugs to directly treat this.
These two groups get streamed differently for APOB goals.
The issue is those in the middle - very disconcerting that someone with 50 Lp(a) would go up to 180. Just shouldn’t be the case. So my take away learning point on this, for my practice, is that those in the middle area might benefit from periodic checks of Lp(a).
Very interesting dialogue, and I think I’ll change one of my clinical approaches on this issue, thanks to the group for sharing the data.
IMO: The people who need to be retested are in the minority.
You need to check your Lp(a) once to see what group you are in; group A with low genetic Lp(a) or group B, with a genetically higher Lp(a). As I have posted earlier with studies to back this up, this is primarily a genetic factor and you cannot do much to move the needle. Focus on APoB instead.
IMO: Forget about Lp(a) and focus on lowering your APoB and doing lifestyle and/or dietary changes if you are not already doing the most you can.
The truth is, as much as it hurts, is that people with high Lp(a) are going to have to work a little harder on life extension interventions than people with low Lp(a).
@desertshores I agree with you in general. But depending on my actual best estimate of my true Lp(a) I would likely put more of my energy and resources on CVD prevention vs other health intimation.
Eg at the higher of my measured Lp(a) levels I’d take the time to see if Pradulent would have a bigger impact on my Apo B and Lp(a) than Repatha, etc
While if my Lp(a) actually is in the green zone as some of my measurements suggest, then I’d focus more on cancer and AD prevention, etc.
So as it’s not crazy expensive I’ll continue to just add on Lp(a) now and then when I get blood work to build out more estimates and help me calibrate whether I’m actually high or low.
At this point I’m also really interested to figure out if there’s some unrealized variable during my past LOWER Lp(a) scores that accounted for such a large drop during those times (other than simple lab error) because obviously I’d want to start taking/doing whatever it was again!
I got a recent blood panel as part of my testing prior to starting rapamycin and acarbose. I added things that I learned about here to make it more complete. So what I added to the basic panel, was Lp(a), ApoB, ApoA1, HbA1c, Cystatin C, Insulin, 25 hydroxy Vit D, Homocysteine, Testosterone-total and free, PSA, and ferritin (HsCRP and GGT were already included). I had also just taken an OmegaQuant test for Omega 3s.
Unfortunately my Lp(a) came back quite high ( 119 mg/dL ) so 2 weeks later I retook the test at another lab. That also was high ( 195.5 nmol/L ). So I just started with atorvastatin at 10mg every other day, if no side effects, I’ll go to 10mg every day. My ApoB was 87 and ApoA1 was 148. Haven’t decided on adding daily low dose aspirin. I’ll wait to start rapamycin after I evaluate the statin.
Enough that “European Atherosclerosis Society consensus statement” now says:
Lifestyle interventions have minimal impact, but a low carbohydrate/high fat diet may decrease levels by 10–15%.31,32
If that is on average some people might get much more (even if others would get much less?)
(Anyone know if they actually are the main, real society?)
Influence of non-genetic factors
Although less well-characterized, non-genetic factors may also modulate Lp(a) concentration (Table 1, for extended discussion see Supplementary material online).31–62
@Neo I don’t think you need to be that extreme, i.e. do keto, to see an effect on Lp(a). The point is that macros matter. Changing the macros for carbs and fat will likely have an effect, without having to go so far as keto. I think it’s worthwhile for each person to experiment with different mix of carbs and fat and see how that changes their Lp(a).
Tell me if I’m wrong, as I’m definitely not an Lp(a) expert. If you have normal cholesterol and LDL levels, is it possible for Lp(a) to be high? And even if it is, do you need to do anything about it?
@KarlT Yes, you can have normal TC and LDL, and have high Lp(a). I have that, unfortunately. I personally would like to lower Lp(a), if I can, because it’s an independent risk factor, apart from TC and LDL.
From the OUP paper @Neo posted above:
“The relation between Lp(a) concentration and these outcomes is continuous; elevated Lp(a) is a risk factor even at very low LDL-C concentration.”
" In a large primary prevention study, the association between Lp(a) and cardiovascular risk was abrogated at LDL-C <100 mg/dL. This finding should be interpreted cautiously, however, given limited patient numbers and potential over-correction of LDL-C for Lp(a) cholesterol. In contrast, the JUPITER trial showed that the association between baseline Lp(a) and first incident cardiovascular event was similar above and below median LDL-C (110 mg/dL), and even at low LDL-C levels (54 mg/dL), reinforcing high Lp(a) as a contributor to residual cardiovascular risk."
I just started a statin to reduce my LDL-C but it appears the increased risk will remain and Lp(a) may even go up. However it appears that lower ApoB from statins lowers your overall risk. PCSK9 inhibitors will lower Lp(a) and ApoB and look like the best solution at the moment (I believe @Neo is using this). Hopefully, as @adssx has talked about, obicetrapib is the solution we need as it is taken orally and seems to be the most effective for Lp(a). The trails I think show that it reduces Lp(a) by a substantial amount. What they’re still waiting to see is if it reduces ACM or heart disease deaths.
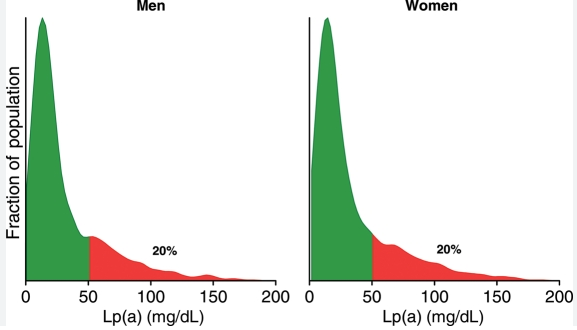
The distribution looks like this in the general population.
(reminder that Lp(a) is six times more atherogenic than LDL-apoB, and no being insulin sensitive won’t change your risk from Lp(a) or apoB. Nada. Zero).
Not sure about the safety profile, but seems to be approved for a form of juvenile arthritis. Actemra has a boxed warning for risk of serious infections.
30-40% Lp(a) lowering, and some IL-6 lowering too are perhaps big upsides.
Anyone have thoughts or know more about this for Lp(a) reduction?
Tocilizumab (Actemra)
Tocilizumab (Actemra) is a biologic medication approved to treat adults with moderately to severely active rheumatoid (RA), adults with giant cell arteritis (GCA), adults with systemic sclerosis complicated by interstitial lung disease, and people ages 2 and above with polyarticular juvenile idiopathic arthritis (PJIA) or systemic juvenile idiopathic arthritis (SJIA). Tocilizumab blocks the inflammatory protein IL-6, which improves joint pain and swelling from arthritis and other symptoms caused by inflammation.
Just went generic in the US, so price my fall drastically and similar in Europe mid last year:
On 29 September 2023, the US Food and Drug Administration approved Tofidence (tocilizumab-bavi) as the first biosimilar to Actemra (tocilizumab). Tofidence is first-of-its-kind biosimilar tocilizumab to receive approval in the US.
And
Europe, the first tocilizumab biosimilar approved is Fresenius Kabi’s Tyenne. This was approved in July 2023 and is available in both subcutaneous and intravenous formulations