Another paper in Nature Aging out today, June 19, 2024 on that even mild CR seems good for longevity:
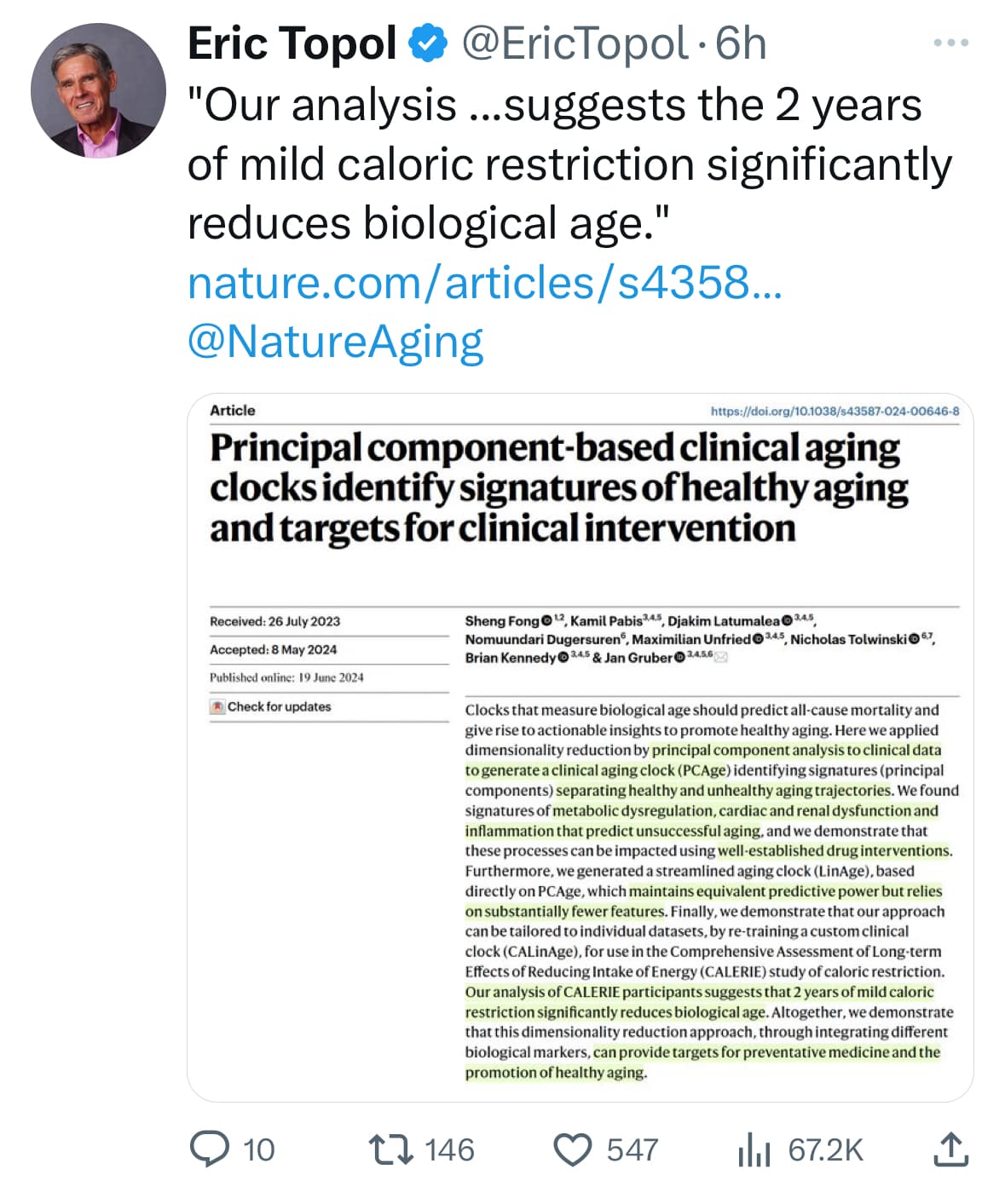
https://www.nature.com/articles/s43587-024-00646-8
See also
Another paper in Nature Aging out today, June 19, 2024 on that even mild CR seems good for longevity:
https://www.nature.com/articles/s43587-024-00646-8
See also
Sorry for not reading the paper but is this CR a long-term thing so that participants weight stabilize on the new lower calorie intake? Or is it inducing a weight loss from excessive body fat or from normal body fat? I’m trying to understand the two factors: autophagy vs losing excessive fat driving metabolic dysfunction.
Also, was there a change to there diet such that people were eating less of the shitty food they normally consumed or were they eating less of the healthy food they previously consumed?
Thanks! I am never going to try to live on as few calories as possible but I am definitely trying to lose a bit of excess visceral fat.
@Joseph_Lavelle Here are some partial answers to your questions
We aimed to investigate the short-term and long-term effects of calorie restriction with adequate nutrition on these risk factors in healthy, lean, or slightly overweight young and middle-aged individuals.
Methods: CALERIE was a phase 2, multicentre, randomised controlled trial in young and middle-aged (21-50 years), healthy non-obese (BMI 22·0-27·9 kg/m2) men and women done in three clinical centres in the USA.
Individuals in the calorie restriction group achieved a mean reduction in calorie intake of 11·9% (SE 0·7; from 2467 kcal to 2170 kcal) versus 0·8% (1·0) in the control group, and a sustained mean weight reduction of 7·5 kg (SE 0·4) versus an increase of 0·1 kg (0·5) in the control group, of which 71% (mean change in fat mass 5·3 kg [SE 0·3] divided by mean change in weight 7·5 kg [0·4]) was fat mass loss.
Calorie restriction caused a persistent and significant reduction from baseline to 2 years of all measured conventional cardiometabolic risk factors, including change scores for LDL-cholesterol (p<0·0001), total cholesterol to HDL-cholesterol ratio (p<0·0001), and systolic (p<0·0011) and diastolic (p<0·0001) blood pressure.
In addition, calorie restriction resulted in a significant improvement at 2 years in C-reactive protein (p=0·012), insulin sensitivity index (p<0·0001), and metabolic syndrome score (p<0·0001) relative to control. A sensitivity analysis revealed the responses to be robust after controlling for relative weight loss changes.
Interpretation: 2 years of moderate calorie restriction significantly reduced multiple cardiometabolic risk factors in young, non-obese adults. These findings suggest the potential for a substantial advantage for cardiovascular health of practicing moderate calorie restriction in young and middle-aged healthy individuals, and they offer promise for pronounced long-term population health benefits.
Here is the original paper that focuses more on the trial details and the participants than the two paper out today on the biological aging measurement:
@Neo thanks
“ for this study, men had particularly high percent body fats for men (26.0 ± 0.6) and moderately high percent body fats for women (36.3 ± 0.5)”
According to Dr Loh, these participants were, on average. obese as defined by body fat percentage. The question would be the amount of visceral fat, which would be driving metabolic dysfunction. Losing all or some of the visceral fat would definitely improve health.
I cannot tell if a constant CR is the key. I hope not. I’d guess that higher physical activity, higher muscle mass, better sleep, and an average calorie deficit over time (until healthy body fatness is achieved) are the key elements. My followup episode with Dr Loh will be published this weekend. She speaks to these elements.
Here’s the relevant methods section on the CR being practiced. It sounds like they were shooting for 25% CR, only hit 12% on average but still saw strong CVD benefits. (I could do 12%!)
One important application for aging clocks is to evaluate the impact of intervention strategies on BA. The CALERIE phase 2 randomized controlled trial was designed to test the effects of moderate (25%) calorie restriction (CR). A cohort of 220 healthy non-obese volunteers between the ages of 20 years and 50 years were randomly assigned to either CR or ad libitum (AL) control groups and followed over 2 years55. Although, in practice, subjects from the CR group achieved only relatively moderate CR (12%), this nevertheless resulted in a significant reduction in several known CVD risk factors56
Coincidentally I have been using a ~12% calorie reduction based on the average of various online calculators.
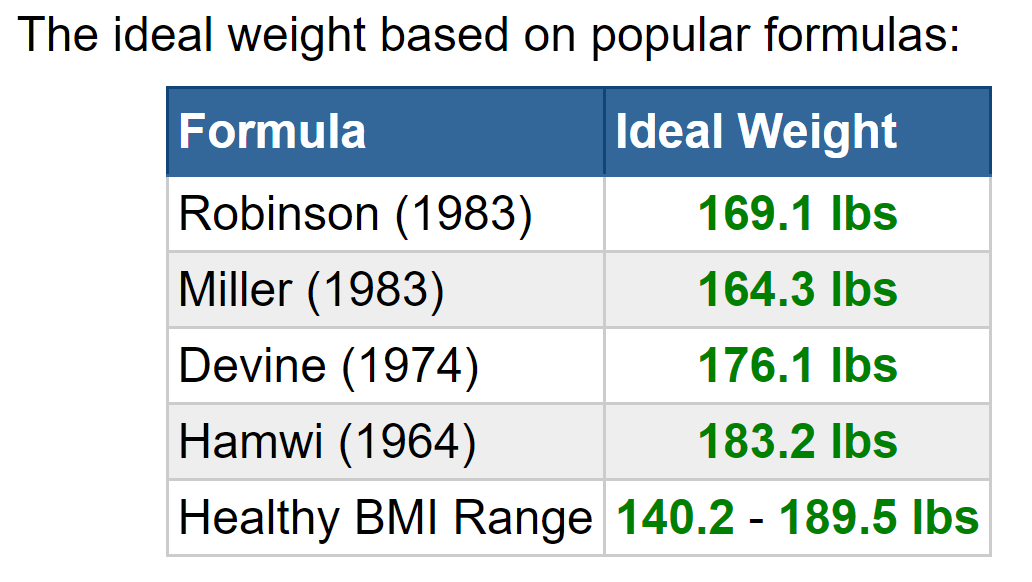
I am surprised that using a calorie restriction calculated from my age activity etc reaches a stasis. Has my metabolic rate slowed down? I have maintained a body weight of 175 lbs. for a long time with little fluctuation. BTW this is my Devine weight. ![]()
After starting rapamycin I lost weight in the first few months and seem to have reached stasis.
Well how is LinAge different from PhenoAge/GrimAge and why does CR help LinAge but not the two others?
Not sure. From much of the mechanistic aging literature it might or even appears to be that good want it at least a material portion of the time.
Yes, transition to better body composition and having had a period of autophagy, IGF-1 down, mTOR down, other key nutrient sensing pathways dialed towards longevity instead of towards growth, etc that can be had from a transient period of CR should be valuable as you suggested.
At the same time for maximal effect, one might have either do it most of the time or at least come back and re-enter that state meaningfully often and for a meaningful percent of the time.
(Anecdotally it seems that Michael Lustgarten and the Blueprint medical team/Bryan Johnson have reached that conclusion).
The Yale professors behind the above NIH funded CR clinical trial and/or Prof Longo and/or Prof Fontana could be amazing people to discuss these questions with - perhaps at some point they could be part of your podcast even…
The classical papers (and books) by Roy Walford that Matt Kaemberlin often refers to might also help shed some light on your question.
Besides this latest clock, LinAge, the mild, short term CR study also found it impacts the third generation clock, DunedinPace. Other methylation studies have also found positive impacts from CR.
Generally, think it’s about what the different clocks are designed to be able to pick up and the limitations of the older, second gen clocks and what they hence are not able to pick up.
The key thing is that the latest (third generation) clocks like Dunedin are PACE clocks - they are designed to identify the rate of aging*.
The older, second generation clocks like Pheno and Grim are AGE clocks, they are designed to predict total, cumulative biological age.
So Dunedin provides a short term, current snap shot of raging rates, while Grim and Pheno are the cumulative effects of a person entire lifetime.
Caloric restriction (CR), defined as lessening caloric intake without depriving essential nutrients4, results in changes in molecular processes that have been associated with aging, including DNA methylation (DNAm)5,6,7, and is established to increase healthy lifespan in multiple species8,9
https://www.nature.com/articles/s41467-017-00607-3
https://www.cell.com/cell-metabolism/fulltext/S1550-4131(17)30168-7?
You are right that this mild, 2 year (so not yet long term) CR study found that:
CALERIE intervention slowed the pace of aging, as measured by the DunedinPACE DNAm algorithm, but did not lead to significant changes in biological age estimates measured by various DNAm clocks including PhenoAge and GrimAge.
At the same time
However, these DNAm measures were developed using different methods and reflect different models of aging. The PhenoAge and GrimAge clocks [both only second generation clocks] were developed to predict mortality risk at a single timepoint in mixed-age and older adults. This approach quantifies aging as a static construct of risk accumulated across the lifetime. In contrast, DunedinPACE [a third generation clock] was developed to predict multi-system physiological decline over two decades of follow-up from early adulthood to midlife. This approach quantifies aging as a dynamic construct reflecting change in risk accumulation.
Said differently
A third generation of DNAm measures of aging are referred to as pace-of-aging measures. In contrast to first- and second-generation DNAm clocks [such as PhenoAge and GrimAge], which aim to quantify how much aging has occurred up to the time of measurement, [third generation clocks like DunedinPACE] pace-of-aging measures aim to quantity how fast the process of aging-related deterioration of system integrity is proceeding.
DunedinPACE may therefore be more sensitive than PhenoAge and GrimAge to changes induced by 2 yr of CALERIE intervention.
Treatment effect estimates may therefore represent a lower-bound of the true impact of CALERIE intervention on biological aging.
Our dose–response and TOT analyses indicated that participants who achieved higher doses of CR experienced more pronounced reductions in DunedinPACE.
The finding that CR modified DunedinPACE in a randomized controlled trial supports the geroscience hypothesis, building on evidence from small and uncontrolled studies14,15,16 and contrasting with reports that biological aging may not be modifiable17
Above is from this paper published last year by Yale in Nature Aging - it’s a good read about both CR and how to think about first vs second bs third generation clocks and how they can be used in clinical clinical trials (and in N=1 biohacking):
https://www.nature.com/articles/s43587-022-00357-y#ref-CR5
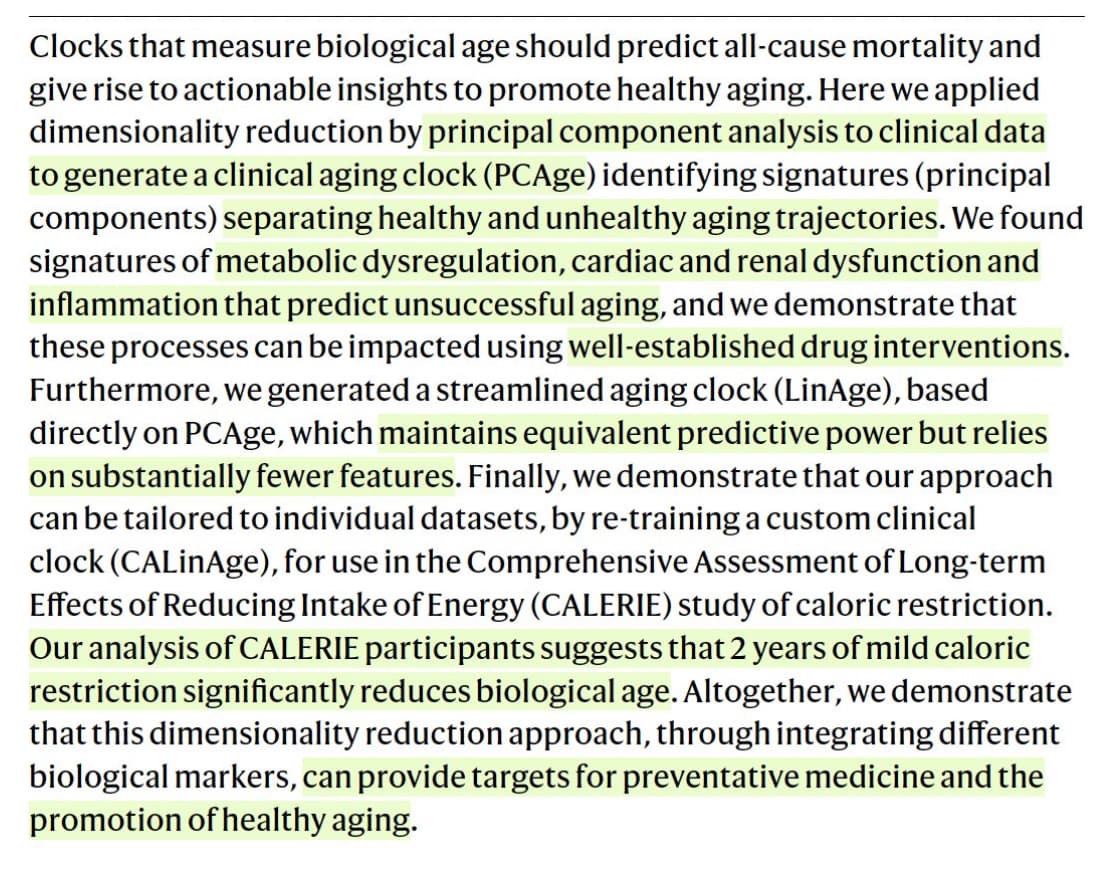
And now there is also the new clock published this week showing effect of even just the mild CR: 2 years of mild caloric restriction significantly reduces biological age
See also here for a lot of color how these later, 3rd gen rate of aging clocks have a lot of advantages vs the older 2nd gen cumulative amount of age clocks:
@Neo thanks. It’s a worthy topic for investing attention.
As you say, I should pose my questions to the experts in the field. I will plan to do that. Right now my mind is wondering about the importance of the living on as little calories (or maybe just protein) as possible. And what does “possible” mean? Certainly there are underfed people who continue living but who are not healthy (or healthy enough to live a good life).
So how can we determine what is too much calories or protein even if body fatness is good (no metabolic issues)? And how do we determine what is too little calories or protein (RED-S issues for example)? And how do we really know if this is a thing or are the studies confounded by test subjects who are benefiting from losing body fat or the tests are too short to tell if too little calories is causing a RED-S type problem or a sarcopenia type problem?
For now I am just focusing on getting my body comp as good as possible by feeding (and more) to reduce visceral fat while maintaining muscle mass and quality. I will try to learn more about this topic.
For contex, here is a post that continues to shape my thinking. From a video of Luigi Fontana MD
Sounds good - will be amazing to listen to any such future podcasts.
One thing, that may be interesting when you look into things is that similarly to rapamycin (and perhaps in even more studies), CR has shown maximal lifespan extension across a massive evolutionary distance and across many, many types of species.
Yes, totally believe in a U shape here! (Edit: But almost everyone in the western world is at the point where less calories likely still would be good for longevity and very few overdo it on the other end of the U).
@Neo We are experimenters here so each of us can make our bets. I am currently heavily influenced by Matt Kaeberlein on this topic who always says not every animal model shows improvement with CR, that people don’t live in laboratory cages (IRL gives lots of need for immune health), and no one can ask the mouse how it feels about CR.
My bet is on cycles of calorie surplus and calorie shortage. My bias is that CR sounds like a shitty life.
100% that we all our figuring out our own paths
I’m just trying to convey my best thinking on what likely works / how does aging work based on my understanding of what the world knows today
I personally do actually not do a lot of CR at this point, perhaps hovering about -10% half of the time and around 0% the rest of the time
But that is because of the enjoyment value of eating / avoidance of hunger feelings (that I totally agree with you on) and not because I don’t think that a Michael Lustgarten / Bryan Johnson / Oliver Zolman approach of a bit more CR would be more physically optimal for my longevity.
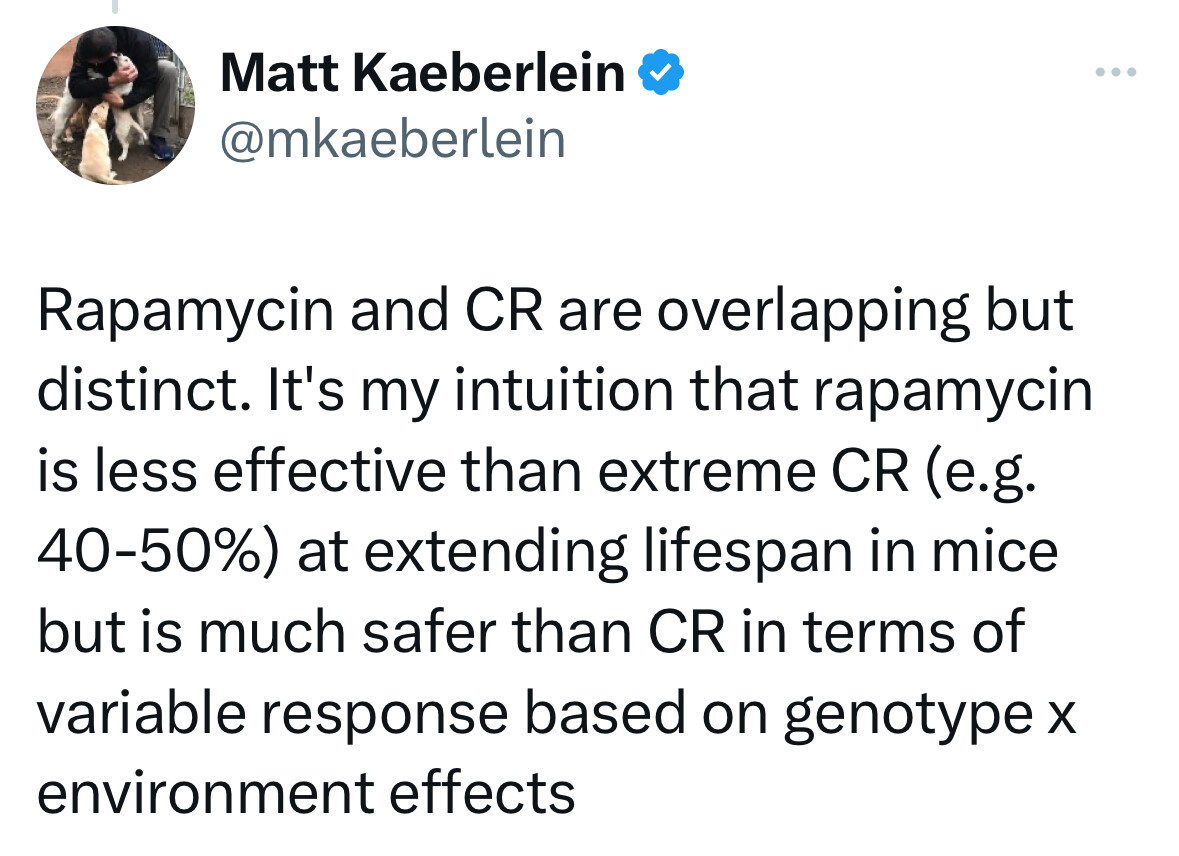
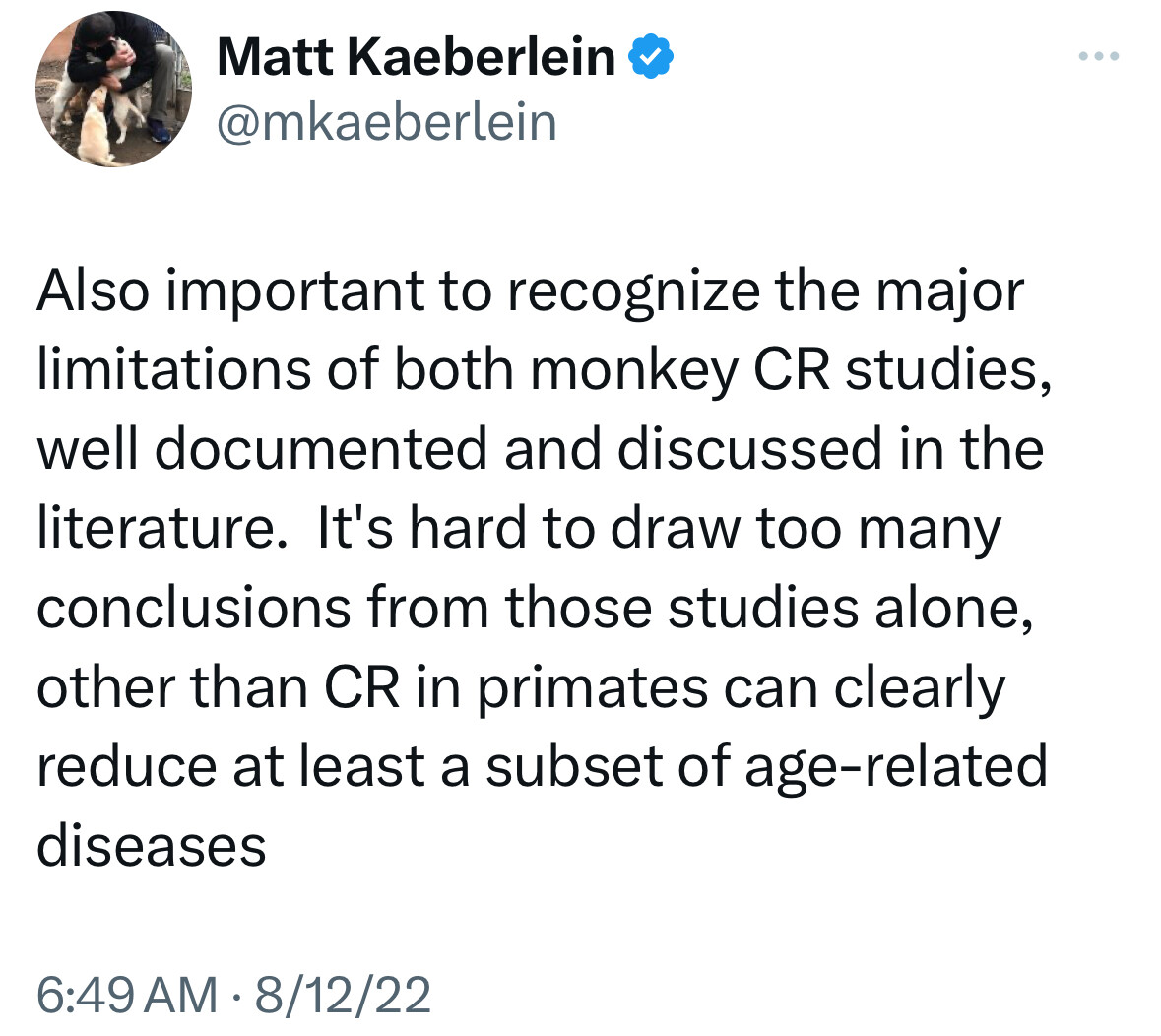
Btw, not sure how much it’s worth, but I think we have a bit different read on Matt Kaeberlein’s view on CR.
I agree that he sees potential safety and adherence issue for humans of extreme levels of CR a la the extreme mouse max lifespan studies
But he clearly often talks about CR as one or even the best supported max life span increasing mechanism I the literature
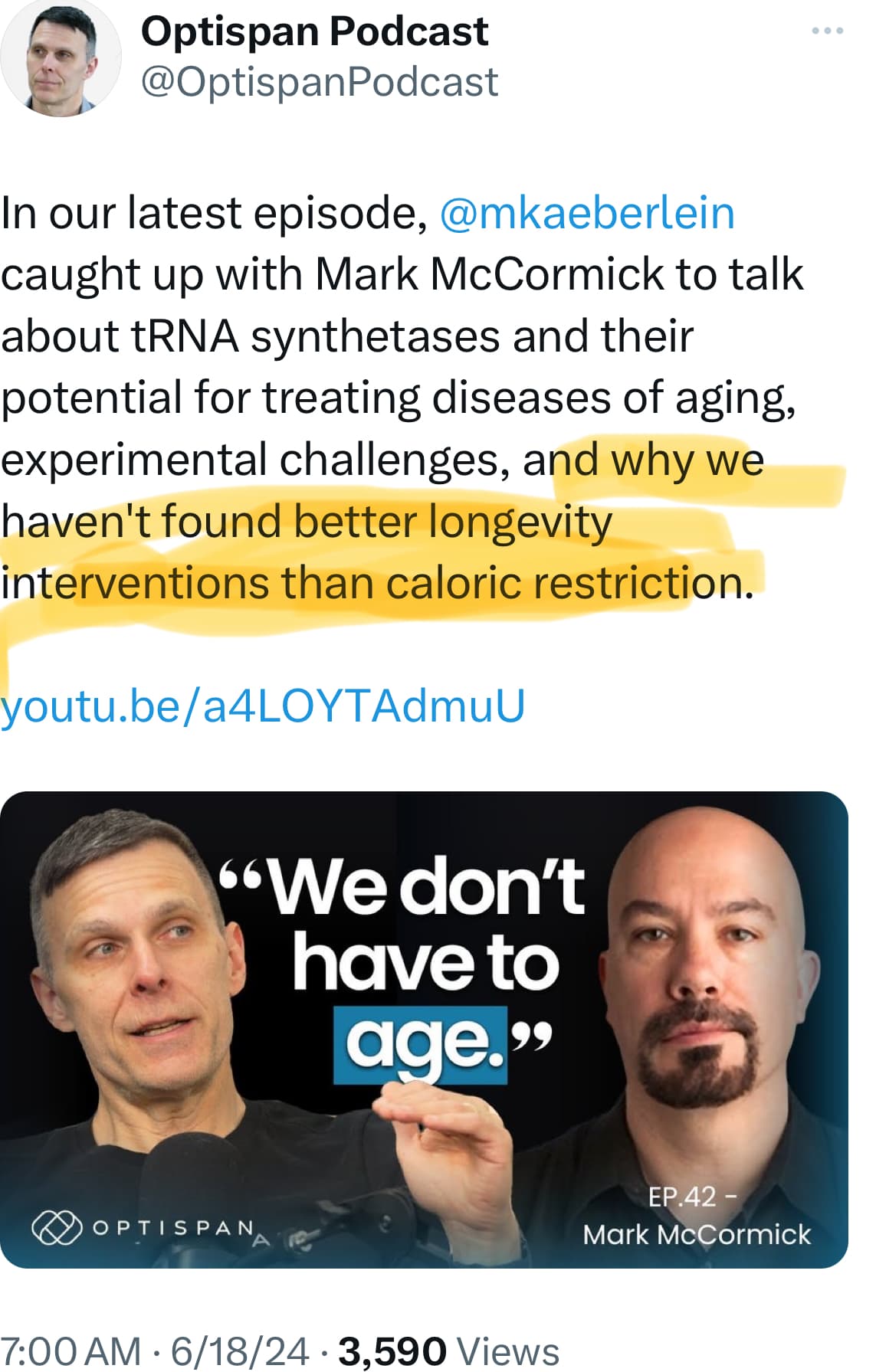
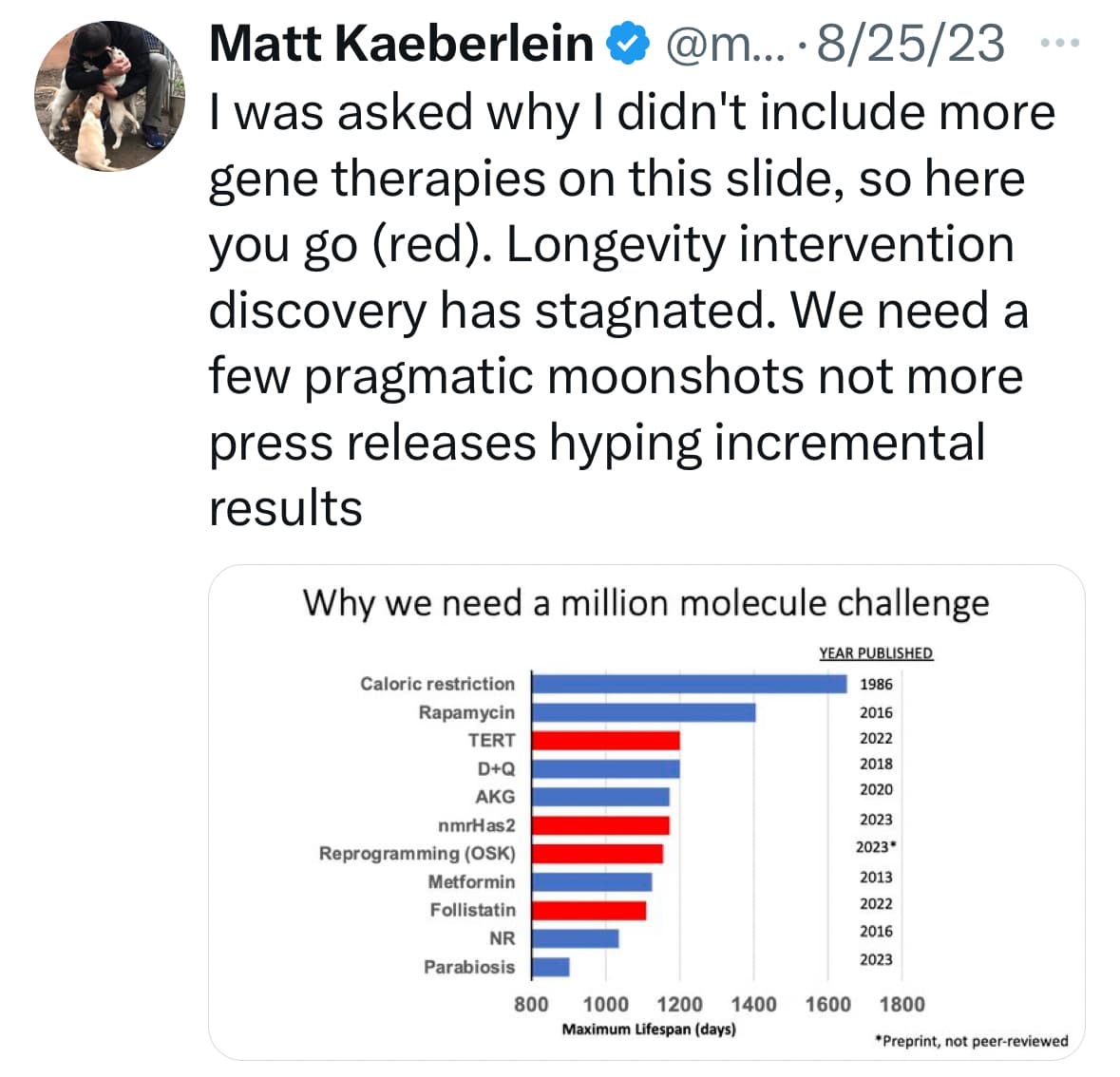
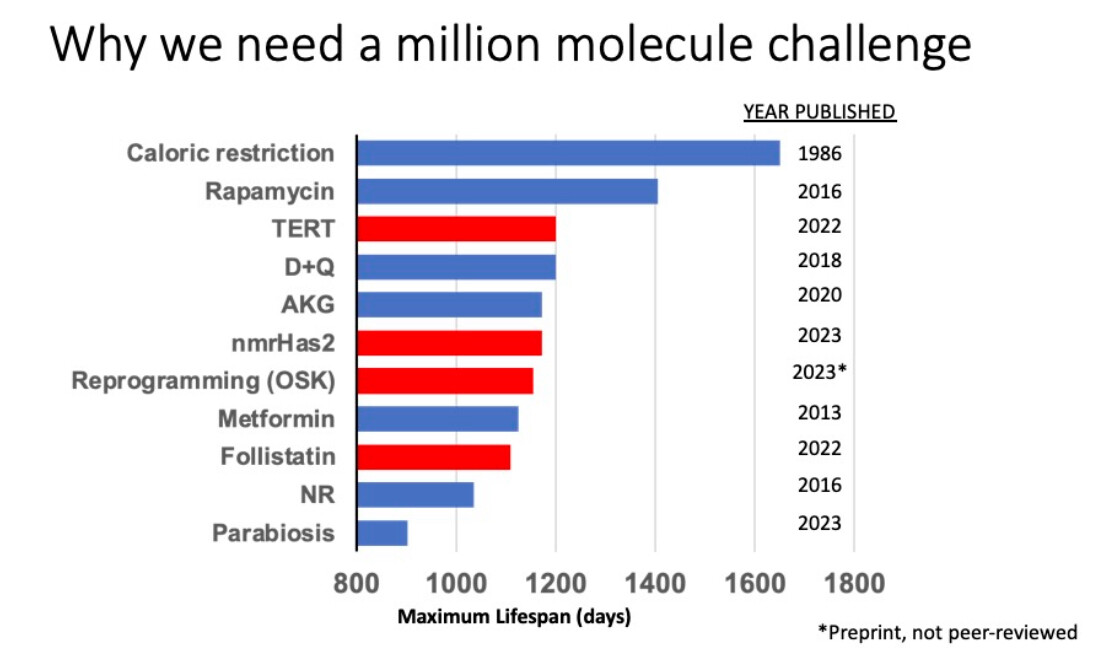
Just this week:
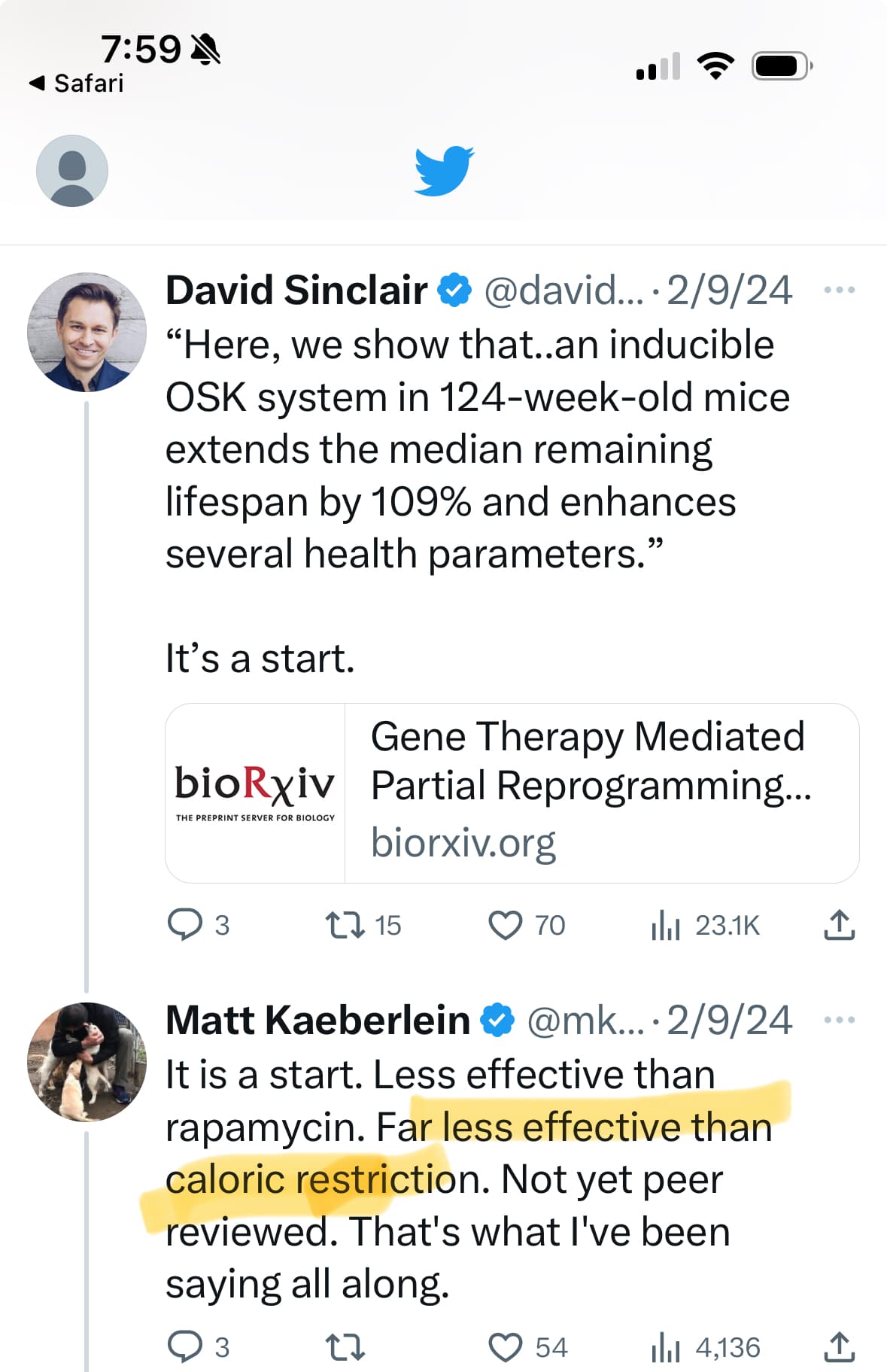
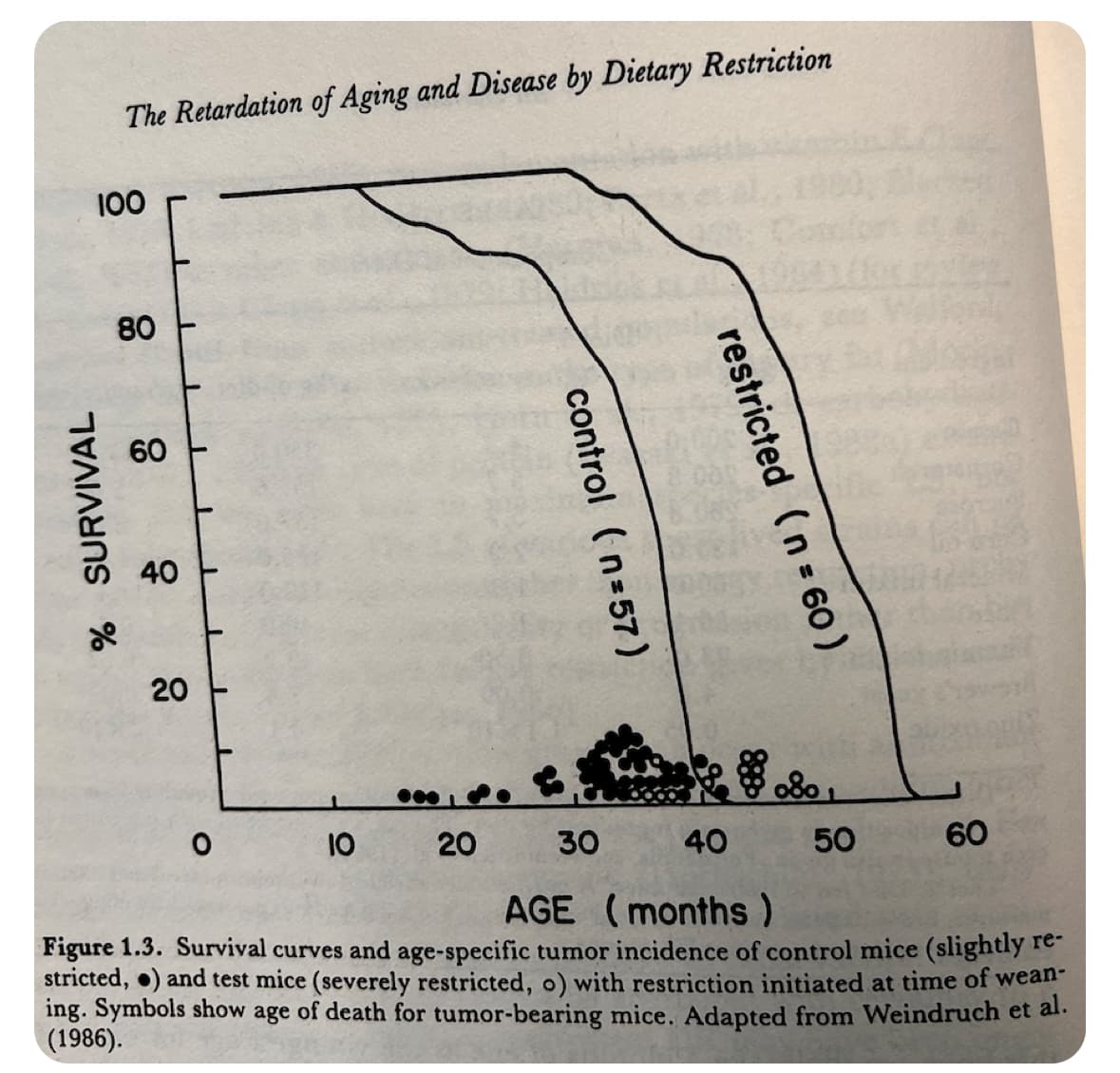
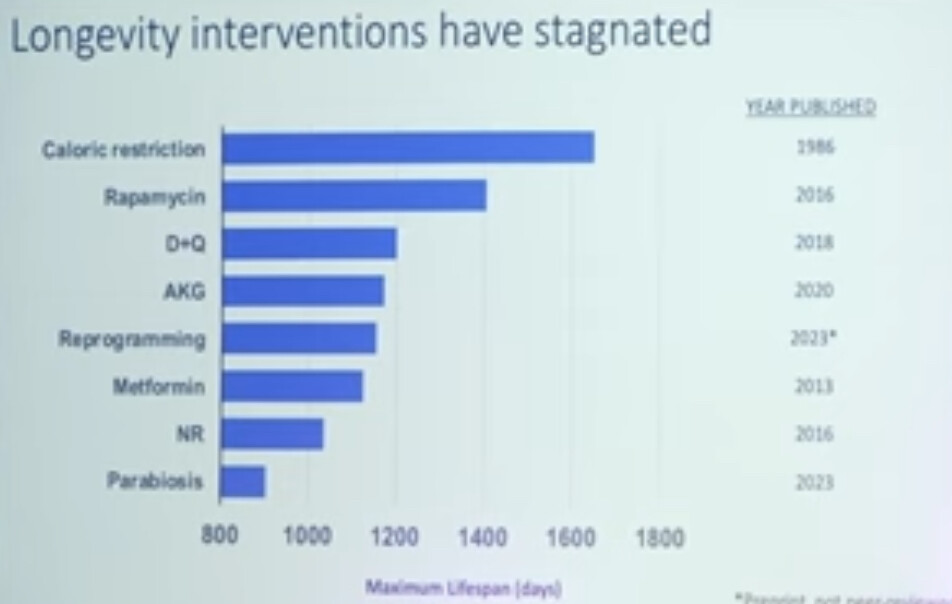
And this chart he often uses:
“My bias is that CR sounds like a shitty life.”
Not for everyone.
At the age of my retirement, I was overweight.
I lost the weight by using a keto diet and intermittent fasting. The reason it was great for me is because (maybe my Scandinavian background) is that I generally don’t like vegetables and fruit.
Some people find it hard to skip breakfast but I didn’t. I didn’t like eating breakfast even as a child.
I eat two meals a day between 12 and 6 PM. I think intermittent fasting might shrink your stomach a little bit, because I now have to force myself to eat enough calories to maintain my weight.
My diet is high in protein with some fat and carbohydrates. I still don’t eat enough protein to agree with some of the studies that say I need so much protein to stave off sarcopenia. The studies may be wrong at least for people taking rapamycin. I have not had any strength or muscle loss that I can detect.
I have the memory of being very hungry after arduous exercise such as playing tennis for hours or hiking, etc. High physical activity results in increased appetite.
That said: I think exercise is as or more important than CR.
The studies lack a comparison with mice forced to use an exercise wheel every day to get fed a non-calory-restricted diet versus mice who were calorie-restricted but not forced to exercise.
@Neo Sure. He says that. But he also says what I’ve repeated. The context is the key. I interpret Kaeberlein as not being a follower of CR
Does CR mean to not overeat, then I agree. Does CR mean to eat so little that the body has to down regulate the immune system and other organ functions? That might also be useful if we have over active function. But surely there is a level so low that is a mistake. It is far safer to cycle it to get the benefits of both retrenchment / autophagy / lower inflammation AND the benefits of growth / strength/ high energy. That’s my bet anyway.
Actually, think you summarized it more correctly here:
—
These probably speak to that question:
Exercise has been shown to protect from many age-related diseases but fails to extend maximum life span in rodents (16, 17, 21).
Although the evidence clearly shows a greater benefit from calorie restriction compared with exercise on longevity, there remains a significant gap in the literature explaining this disparate effect. The effects of calorie restriction (40) and exercise (6) on age-related diseases and markers of aging have been exhaustively studied independently, while only a limited number have examined calorie restriction and exercise in tandem (26, 36).
Rodent (17) and human studies (32) suggest that increasing energy expenditure via exercise fails to mimic the life-prolonging benefit of consuming fewer calories.
These results showed that mild and moderate calorie restriction were more effective at lowering fasting IGF-1 and insulin levels than exercise, and animals on moderate calorie restriction most closely resembled young animals for measures of hormones and stress-related proteins. In contrast, exercised animals were leaner than calorie-restricted mice and exhibited greater tissue levels of HSPs and oxidative phophorylation complex content in skeletal muscle mitochondria.
Thus, it is possible that some harmful byproduct(s) or consequence(s) associated with exercise “interferes” with the beneficial effects of being lean. Alternatively, calorie restriction may extend life span by a mechanism(s) independent of leanness, and exercise may fail to activate these critical pathways to the same scope or magnitude.
Recently, Fontana and colleagues (10–12) have examined systemic biomarkers in individuals on a selfimposed low-calorie or low calorie-low protein diet vs. individuals engaged in high-volume exercise for several years. Despite a similar body mass index (10, 12) or fat content (11), long-term calorie restriction and exercise resulted in disparate effects on various parameters related to aging, including thyroid function, systemic inflammation, and growth factors. For instance, individuals engaged in voluntary calorie restriction were found to have lower levels of serum T3 and TNF-α levels than exercisers or a control group consuming a typical Western diet (11). In another study, individuals consuming a low calorie-low protein diet were shown to have a more favorable cancer risk profile than endurance runners or controls, including lower serum IGF-1 and greater levels of dehydroepiandrosterone sulfate and sex-hormone-binding globulin (10). Furthermore, a low-calorie vegan diet resulted in lower blood pressure than exercisers (12). Taken together, the present investigation, coupled with these related studies in humans suggest that at the same relative energy deficit, exercise fails to completely mimic the beneficial changes associated with calorie restriction.
Therefore, the available evidence demonstrates that an increase in energy expenditure can attenuate disease risk (20, 22) but does not presently support the notion that an energy expenditure-induced energy deficit slows the rate of biological aging (20).
- Rats that exercise regularly will, on average, live longer compared to a group that eats the same amount but does not exercise. This is because exercise prevents some diseases, which allows more individual animals to live out their expected life span.
- However, when comparing the rats in these two groups that eat the same amount, the longest-lived animals in the exercise group don’t live any longer than the longest-lived rats in the non-exercise group. Taken together, these findings indicate that exercise can prevent an early death from disease in some rats, but does not extend the maximal lifespan of any of the rats.
- When comparing rats that exercise to those that don’t exercise but eat much less, the longest-lived rats are from the group that ate less.
For above and more see:
Agree (and I said when agreeing that there almost certainly is a U-curve here).
I can see value to a cycling protocol (but think less data to guide).
Question is what the “highs” should look like in a cyclical protocol? It does not seem to be a binary choice and have to be extreme CR or no CR or extreme CR or surplus calories. It might be that our highs in a cyclical protocol should still be something like what Mike Lustgarten, Bryan Johnson (after he decreased the degree of CR to a more mild CR) and the NIH / Yale CALORIE trial participants on average actually ended up doing - those are much more tolerable/enjoyable and should have less of the in the moment immune system lowering effect.
@neo. I agree that the amplitude of highs and lows matter. Too much protein at once (24 hours?) is just converted to calories to store or burn. Too much of a calorie deficit can lead (me) to overeating once the dam breaks.
I think the main idea is to maintain a healthy body fatness and muscle mass (and organ function) over time but not every day. Stress is good. Recovery is good. Adaptation is good.
I think short cycles of small excess and deficit are best for older people to minimize the muscle losses and to minimize the fat gain…which get harder to compensate for in aging. To get to the ideal body comp is hard. Staying there requires a permanent change in identity… to become the person who lives that life easily. But be careful what you wish for.
Have you seen @ConquerAging diet? I can’t help but think he “likes” it because he is starving. The most delicious meal I ever had was half of a freeze dried Hawaiian pineapple chicken camping meal that a random stranger gifted my climbing partner and I after a 8 hour climb up the Diamond of Longs Peak. I would have eaten an old shoe with cheese on it to be fair.