Place crushed fin tablets in a non-transparent 00 capsule, and some creatine in similar capsules. Have each in a small bag which you mark on the bottom. Take one randomly from one bag, see if you get depressed the next day. Check which bag it was the next day. Repeat a few times.
It is partially off-top, but I think, sometimes we are tooo focused on DHT in terms of BPH. It is part of the puzzle, but the picture is much bigger and includes several key pathways:
5-LOX pathway: The 5-lipoxygenase pathway contributes to prostate inflammation and growth. Inhibiting this pathway may reduce BPH progression.
Inflammation and NRF2: Activating NRF2 (Nuclear factor erythroid 2-related factor 2) can reduce oxidative stress and inflammation in the prostate.
Metabolic syndrome: Addressing obesity, insulin resistance, and dyslipidemia is essential, as these factors are linked to increased BPH risk.
TST/DHT: While healthy levels of TST and reducing DHT can help with BPH, I am still personally and subjectively concerned about continuous substantial decrease of DHT and its impact on neurosteroids like pregnenolone and DHEA (like mentioned in this forum by @Shady many times) (with that → I am personally using intermittently phytochemicals with “anti” 5-alpha-reductase activity, which are reducing DHT, but not so dramatically, like finasteride).
Last but not least and coming back to ezetimibe: recent research suggests cholesterol metabolism plays a role in BPH/PCa development. It seems, that particularly arachidonic acid / cholesterol working here hand in hand. Interesting study Cholesterol: An important actor on the cancer immune scene:
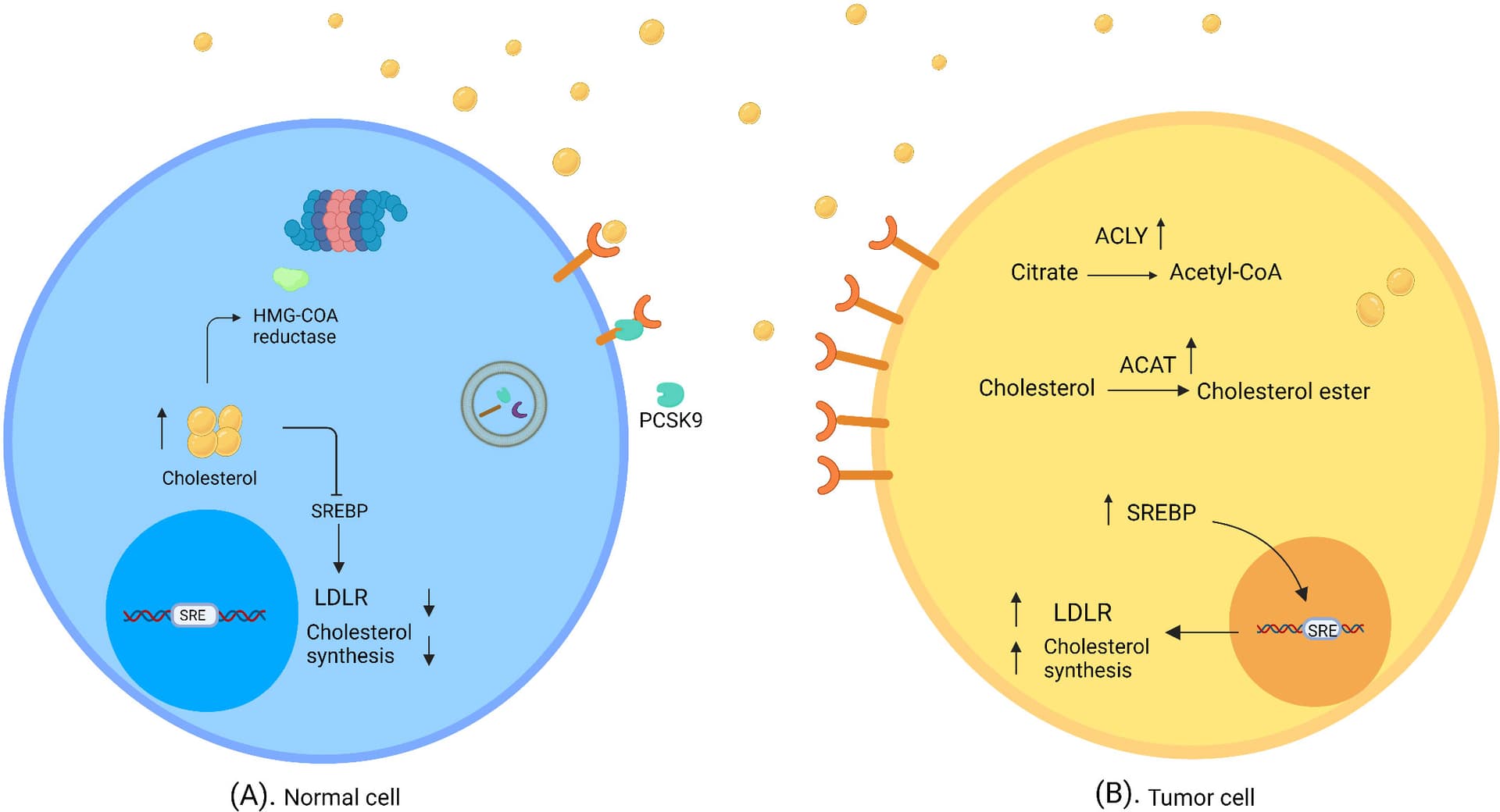
Normal and tumor cells in cholesterol-rich environment. (A) In normal cells, a high concentration of cholesterol triggers regulatory mechanisms of cholesterol synthesis and uptake, which downregulate SREBP and degrade HMG- CoA reductase. (B) Tumor cells evade feedback mechanisms in a cholesterol-rich environment. SREBP shows high activity; thus LDLR expression and/or cholesterol synthesis are elevated. ACAT catalyzes the synthesis of cholesterol ester; therefore, cholesterol accumulates in tumor cells. ATP citrate lyase converts citrate to acetyl-CoA and induces fatty acid synthesis
Cholesterol-rich environments change immune cell phenotypes and functions, such that these cells may support cancer cell survival… Cholesterol can potentially act as a cause or an effect of cancer, although the type and stage of the tumor should not be overlooked.
Which is not an issue with finasteride in humans due to the selective inhibition of the 5ar type 2 enzyme
Personally, I remain sceptical about potential other treatments until they prove to work quite as well as 5ar inhibitors, tamsulosin and tadalafil. Until they have proven themselves in preventing or treating BPH, this post sounds like the BPH-equivalent of “LDL isn’t the cause for heart disease it’s actually carbs”.
@DeStrider interesting video in this context from Attia + Dr. Ted Schaeffer - clinician/researcher in the field of prostate cancer, speaking about PFS. @DrFraser - very much in line, with what you saying - he is not recommending 5ar-blockers as prevention: “But I definitely see it (PFS), so that’s why I never really use it in my practice. I mean, it’s just such a limited drug, in part because its efficacy is limited, in my opinion, in terms of managing lower urinary tract symptoms. Additionally, the side effects, including PFS, are real.” Attia also speaks about potential importance of androgen receptors / DHT…
Dr. Schaeffer can call it a “limited” drug, but it’s not like the alternatives are any better. If your prostate continues to grow it will eventually cut off your bladder’s ability to empty, and I’d imagine you’d die an unpleasant death if you didn’t have access to modern health care. That’s pretty serious. Short of surgery or radiation to shrink the prostate, what else is there? It be great if Ezetimibe can be proven at some point in the future as efficacious in this matter, but for now it’s just hopeful thinking.
And here a response analysis from my favourite hair health youtube.
To also prevent appeal to authority fallacies, here once again the official FDA stance regarding finasteride as of 2022:
The US Food and Drug Administration (FDA) had advised that the PFS petition “does not provide reasonable evidence” of a link to suicide, but in August 2022 added suicidal ideation (SI) and behaviour to the adverse reactions listed for finasteride. According to the FDA statement, the PFS petition “does not provide reasonable evidence” of a causal link between finasteride and persistent SD, depression, or suicide. However, on the basis of reports from patients using the 1-mg dose for AGA, the FDA is “requiring the addition of SI and behaviour” to the listed AEs.
The aim of this study was to evaluate the beliefs and counseling practices among dermatologists regarding adverse effects of finasteride. Anonymous paper surveys were personally distributed to 122 attendees at two annual major dermatology meetings. The participation rate was 82% with 47% women and 77% residents of the United States. 51% of respondents believed that finasteride could cause sexual side effects and 18% believed that it could cause persistent sexual side effects. Fewer than a quarter believed that finasteride could cause depression or lower sperm counts.
Alongside a case study in which PFS is described as a possible delusional disorder.
We report the first case of PFS in a long-standing (over 20 years) dermatotrichological practice with frequent finasteride prescription observed in a 25-year-old male following dutasteride treatment for male androgenetic alopecia. There was circumstantial evidence that PFS may represent a delusional disorder of the somatic type, possibly on a background of a histrionic personality disorder, which would explain the refractoriness of the condition and a high degree of suggestibility.
Why not Dutasteride?
I appreciate the whole PFS stuff may be rubbish - but along with that, if there is another sensible alternative - and there is a little controversy - why not just avoid it. It looks like a lateral move on efficacy and prostate cancer rate reduction.
I am assuming that Dutasteride and Finasteride have similar side effects (e.g., PFS happens to Dutasteride users too) so there’s no benefit to switching. Please correct me if I’m wrong.
That’s not an unfair comment - but dutasteride inhibits Type 1 and Type 2 5-AR and Finasteride mainly Type 2 … the reports … assuming the entity even exists, seem to be a lot less with dutasteride.
I guess I always look at my decisions, as it is for someone else - and they get the benefit or adverse effect of what I recommend - there is a burden when folks have problems and you have to question your own decisions. If there were a good reason for a 5 alpha reductase inhibitor … I’m probably a bit happier to justify the decision if using dutasteride - at the point there is a problem. Again, this is smoke and mirrors … does it exist, doesn’t it? I don’t honestly have the time or interest to be certain. I however have a number of colleagues who have essentially 100% of practice in this realm … they have advice for other physicians. I’m reluctant to ignore that advice - even if not based on published data.
This has been the advice … again - I’m not an expert in this, but for physicians who exclusively work in Men’s sexual health … it was the advice given in a couple of lectures. Of course all of this based upon “expert opinion” for what that is worth?
In a post-hoc analysis of data from 4974 non-statin-using men in the REDUCE (Reduction by Dutasteride of prostate Cancer Events) trial, a team led by Stephen J. Freedland, MD, of Cedars-Sinai Medical Center in Los Angeles, found that each 10 mg/dL increase in serum total and HDL cholesterol is associated with a significant 5% and 14% increased odds of a diagnosis of high-grade PCa, respectively. The investigators found no association between total serum cholesterol and overall or low-grade PCa and between LDL cholesterol and the risk of any PCa.
Particularly: interesting to see HDL in this light…
I have read that dutasteride is more likely to have side effects due to being more powerful but I have consistently heard that dutasteride is “safer”. Of course my doctor hasn’t heard any of these things. It is confusing.
Dutasteride can actually inhibit neurosteroid production in the brain, assuming it crosses the BBB. It inhibits over 90% of serum DHT and between 50-80% of tissue DHT depending in the dose.
Dutasteride also has a very long half life so if you get side effects, you can have them for over half a year until it has cleared your system. Up to 12 months for 2.5mg dutasteride per day which some men are taking due to very aggressive hairloss.
Mechanistically, dutasteride is absolutely riskier than finasteride but somehow the clinical trials have a similiar incidence of side effects. The only two reasons I can think of why it’s considered “safer” is because 1. far less people take dutasteride for hairloss than finasteride and 2. there is no profit-oriented group sueing GSK for Avodart, unlike with the PFS Foundation and Merck.