Wow, that’s fantastic! Congratulations.
1 Like
Thanks, I’m from Belgium and used an Italian product: Benzalip 400mg from Aurobindo Pharma
3 Likes
That’s amazing! I’m definitely going to look for it. My Lp(a) has been steadily going UP for some reason, even though I’m on a PCSK9 inhibitor (along with ezetimibe and bempedoic acid). My LDL is only 33 (awesome), but my Lp(a) is now 175 mg/dL !! ![]()
Just heard back: bezafibrate is not available in India ![]()
1 Like
May I ask what it went up from and over what time period?
Nor is it available in the US. What a bummer.
175 mg/dL? Dang, that is high. Mine is around 175-195 nmol/L
Good thing is whenever one of the new drugs come out, you’d most certainly qualify for it.
1 Like
I have compared all my results from 16 november with those of 16 februari, and found one side effect; my homocysteine increased from 8,6 µmol/L to 11,5. I had lowered it 3 months ago by following this protocol for 3 months;
But now it’s back at the range it was before. I found this in the literature about this effect;
My B6 and B12 levels are optimal and I daily take a methyl folate, methyl B12 and P-5-P (B6) supplement, so I will have to think about what I can do to further optimize. Maybe I 'll try an other fibrate, unfortunately gemfibrozil is not available where I live…
1 Like
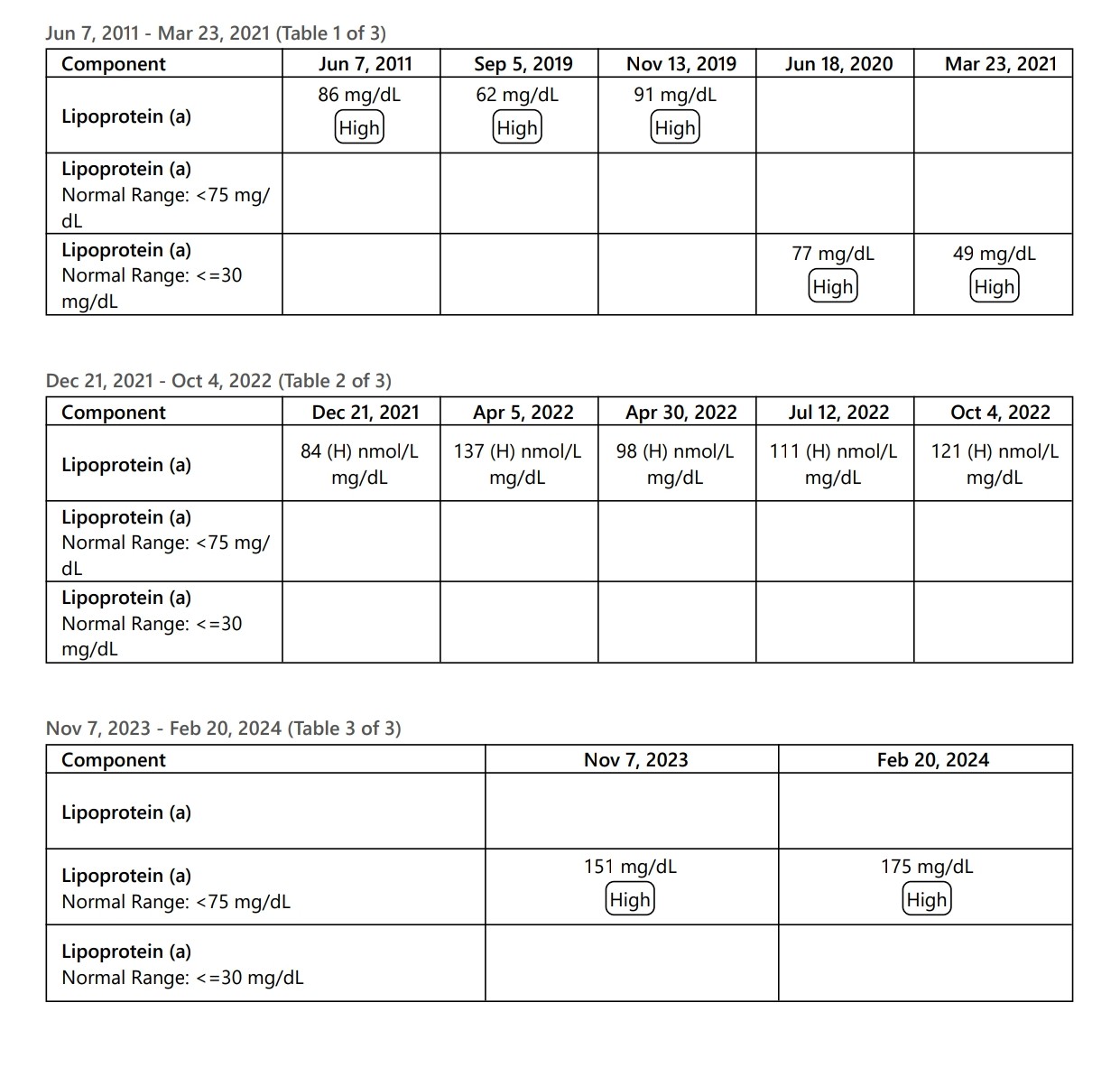
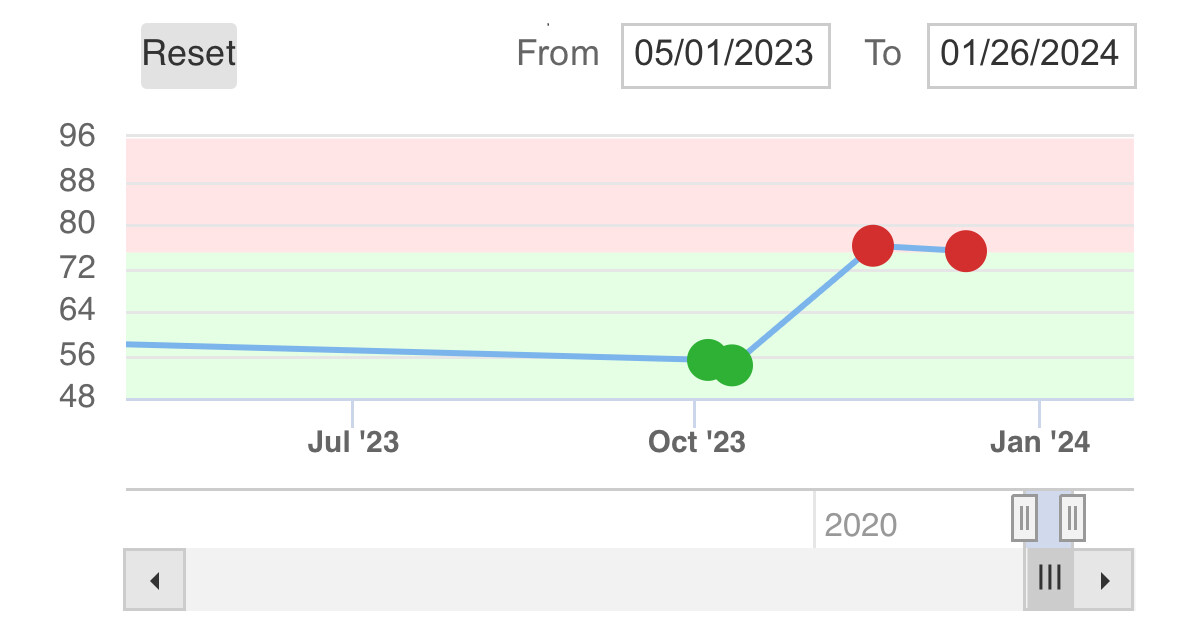
I need to call the lab and speak to their director to figure out WTH they are doing. Attached is my Lp(a) taken at various times over the past 13 years. As you can see, the numbers (and measurement units) are all over the place! Makes zero sense for something is supposed to be stable. There’s no way my Lp(a) has more than tripled from a low of 49 mg/dL in 2021 to a high of 175 mg/dL now.
5 Likes
Wow, yes. This is really strange.
Are you sure than none of them are in mmol/L (roughly a factor of two difference)?
I also had some variability:
Maybe not. Here is my data from Quest on Lp(a)
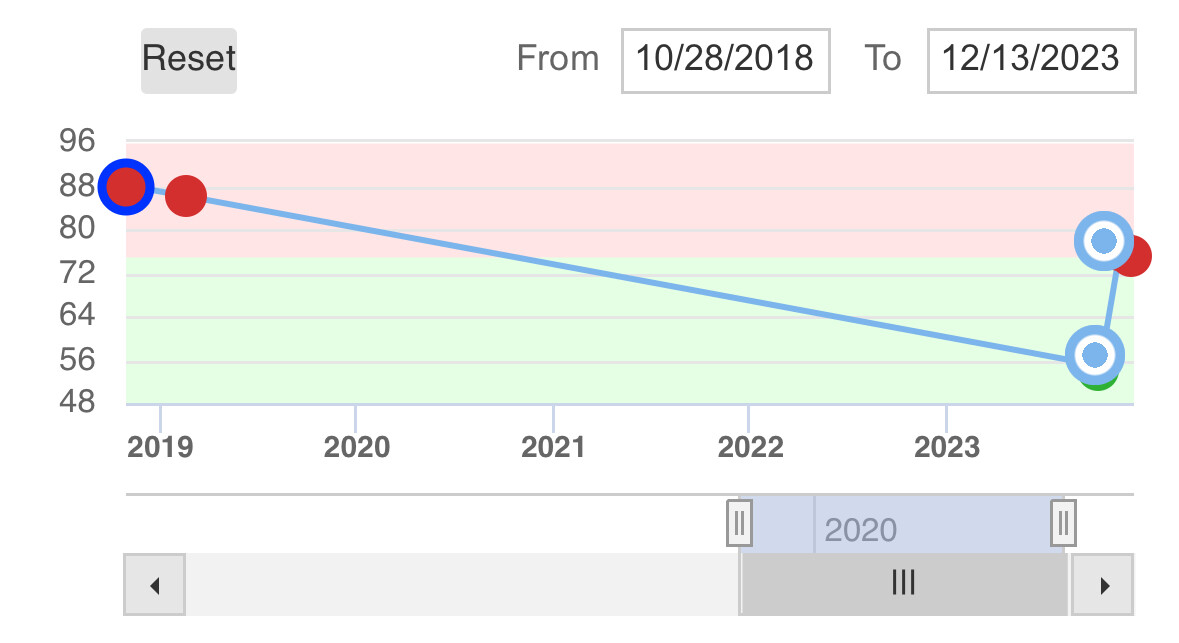
And here is my data from LabCorp:
without being on any cholesterol related med:
(Have a few other data points around that level from LabCorp)
—
And here is from when being on a half dose of Repatha:
From the last two data points there was enough data for my cardiologist and me to ask ourselves if it might be worth trying a full dose of Repatha instead of the half dose. (A half dose lowered my Lp(a) 25%). This is an experiment we are doing right now.
But what if the only Lp(a) blood test we took was the Quest Diagnostics one from October 2 or 6 2023 where the levels were ~55? Those were BOTH from a period when I had not been on PCSK9i or any cholesterol med for many months.
Either I had found some magical way to lower my Lp(a) via diet or exercise or supplemented that there were no know Lp(a) benefits from… or much more likely those two tests has testing errors.
But if we only had one (or even both of those data points) and thought they was my baseline (a) we would be less concern and I may not have pushed for taking PCSK9i and (b) when we then looked at the Quest datapoints from when I was on PCSK9i in November and December at levels around 75 or so, we could have concluded based on data that PCSK9i increased my Lp(a) level by 35-40%….
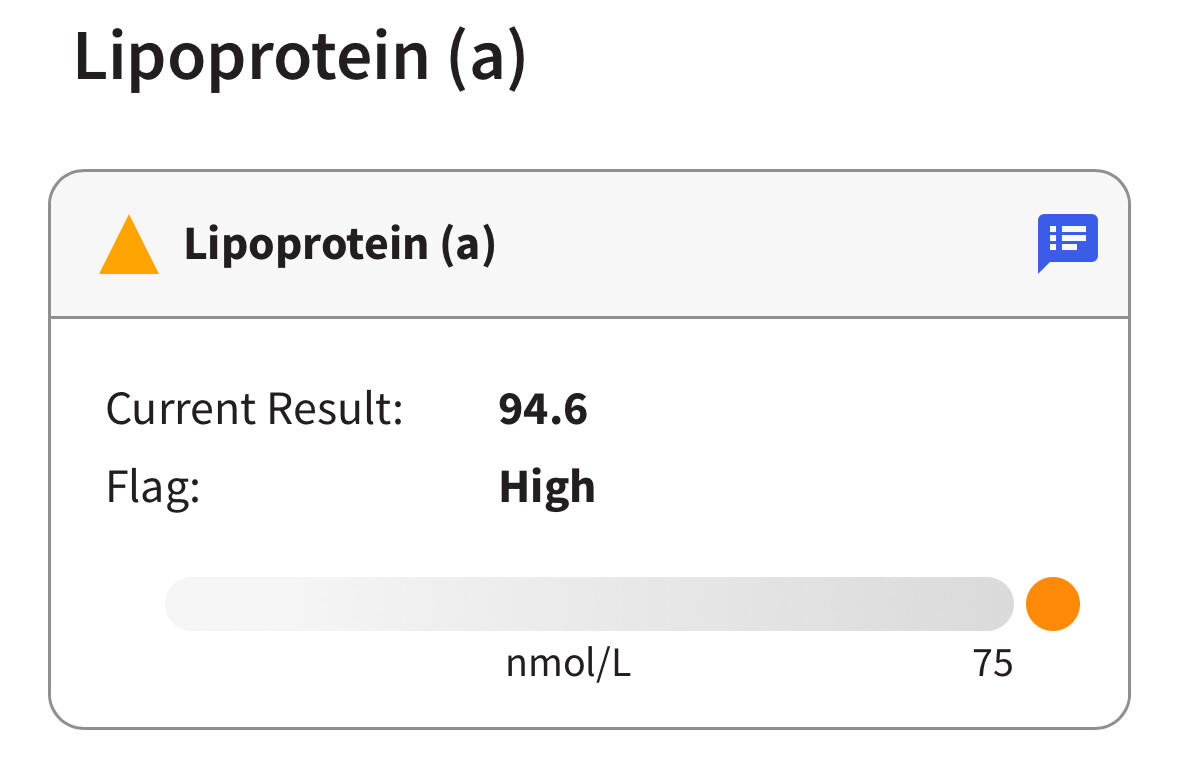
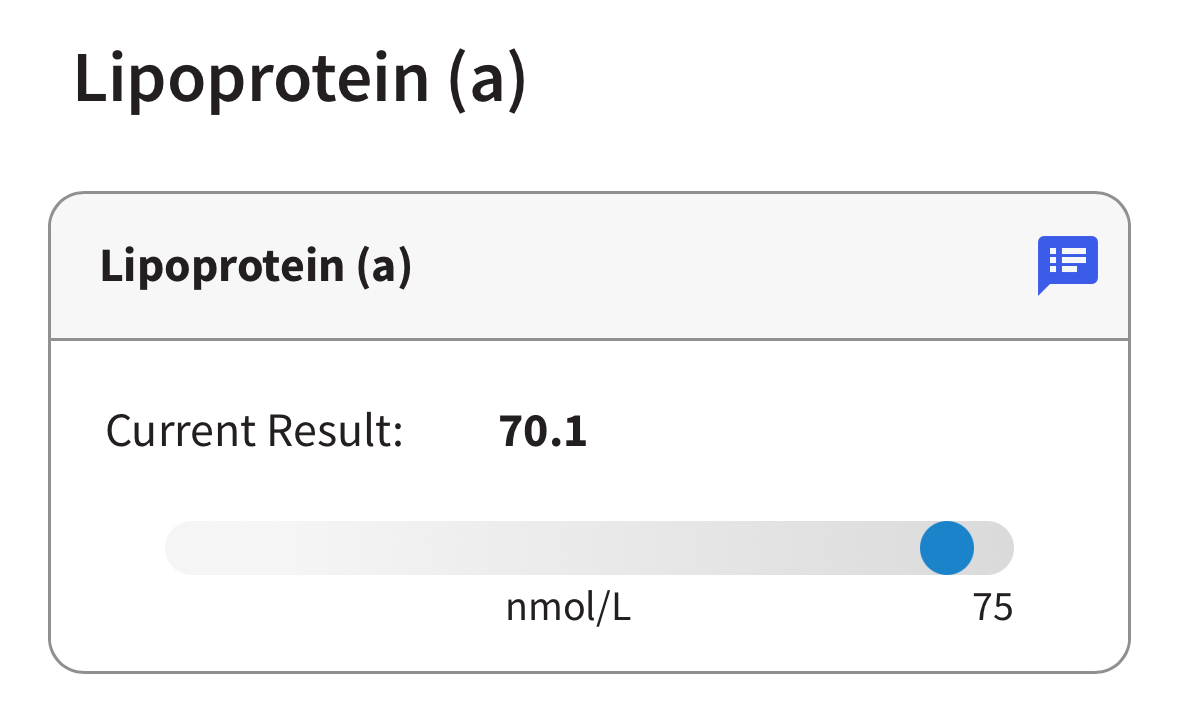
Clearly when we see all the data points it’s almost certainly that I’m around 85-100 when on no medication, and it goes down by perhaps 25% to 70ish whenever I do decreases level PCSK9i.
This is just one example of why we should rely on more than one data point when gathering data to make decisions on.
There is always an error bar around any blood test, so you have to think about any one data point as being within a confidence interval that generally can be quite wide.
3 Likes
If you look back at the chart, several data points are in nmol/L because at one point, the lab announced they were changing to nmol/L since it’s more accurate. Suddenly the last two times I’ve had it measured, they’re back to mg/dL. And mind you, I’m on full dose Repatha. I believe my local lab sends these specimens to an outside lab for analysis, so first thing I’m going to find out is have they been sending to different labs over the years and if so, which lab(s).
I’m also thinking I need to do some research about any differences in Lp(a) testing methodology, which lab uses which, and get my Lp(a) retested (most likely with Quest or Labcorp).
3 Likes
Ok so I called my local lab and figured out they entered the units all wrong, so at least my “175” is in nmol/L not mg/dL (but still way to high!), but it still doesn’t explain why my numbers have gone up from 98 → 111 → 121 → 151 → 175 over just the past 2 years(!!) All tests were done at Mayo Clinic Labs, so I left a message to find out if they’re doing something different with their assay because this just isn’t making any sense.
3 Likes
Just saw this chain of recent comments and was going to suggest the unit issue. It sure looks to be a mix of units. The problem is, you don’t know what they used when, mg/dL or nmol/L. Your table for Dec 21, 2021 - Oct 4, 2022 has both units listed!
The conversion factor is roughly 2.5 x to go from mg/dL to nmol/L. It is not precise because Lp(a) doesn’t have a precise molar mass, or else they could just do it in mg/dL.
But yeah, it’s still confusing because you are effectively back up to 70 mg/dL on your recent test (175 nmol/L) from 49 mg/dL a couple years ago.
5 Likes
Yes, when I look at each result separately, it gives the correct units (nmol/L) for every test done since December of 2021. It’s when I click on the “Trends” button to look at the results on a table (the one I printed out) that the lab somehow screwed up the data consolidation.
Now just have to figure out why the heck the value has increased so dramatically for a test that is supposedly so “stable” over time, especially when I’ve been on a PCSK9 inhibitor since late 2019.
2 Likes
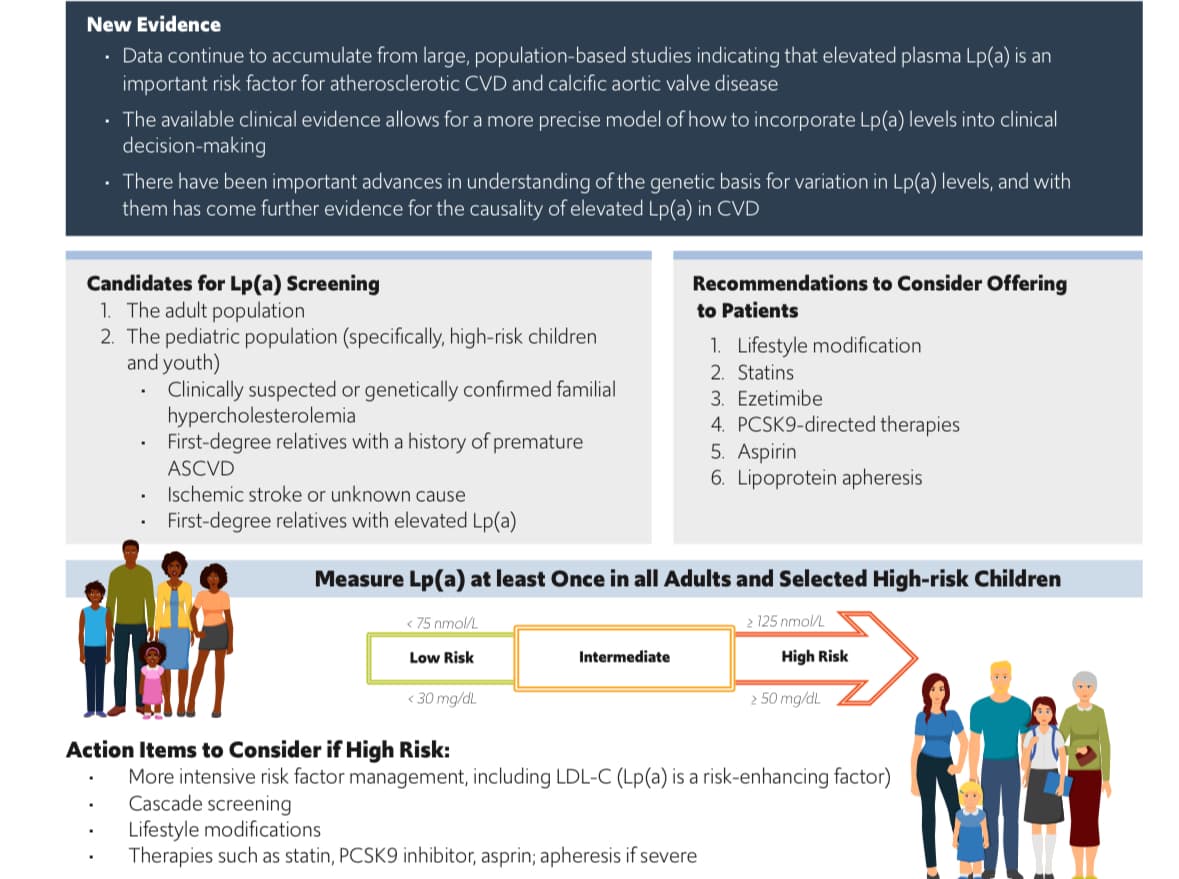
Scientific Statement on Use of Lipoprotein(a) in Clinical Practice
Last Updated: Thursday, 07-Mar-2024 15:00:00 EST
The lipoprotein(a) [Lp(a)] field is rapidly evolving on many fronts, including understanding of the association between Lp(a) levels and cardiovascular disease (CVD) risk in different contexts, and how best to manage other CVD risk factors in patients with elevated Lp(a). Considering new insights into the clinical management of these patients, and in the absence of FDA-approved therapies to specifically lower Lp(a) levels, the question of in whom Lp(a) should be measured has become an increasingly important issue in clinical practice.
Full paper
3 Likes
3 Likes
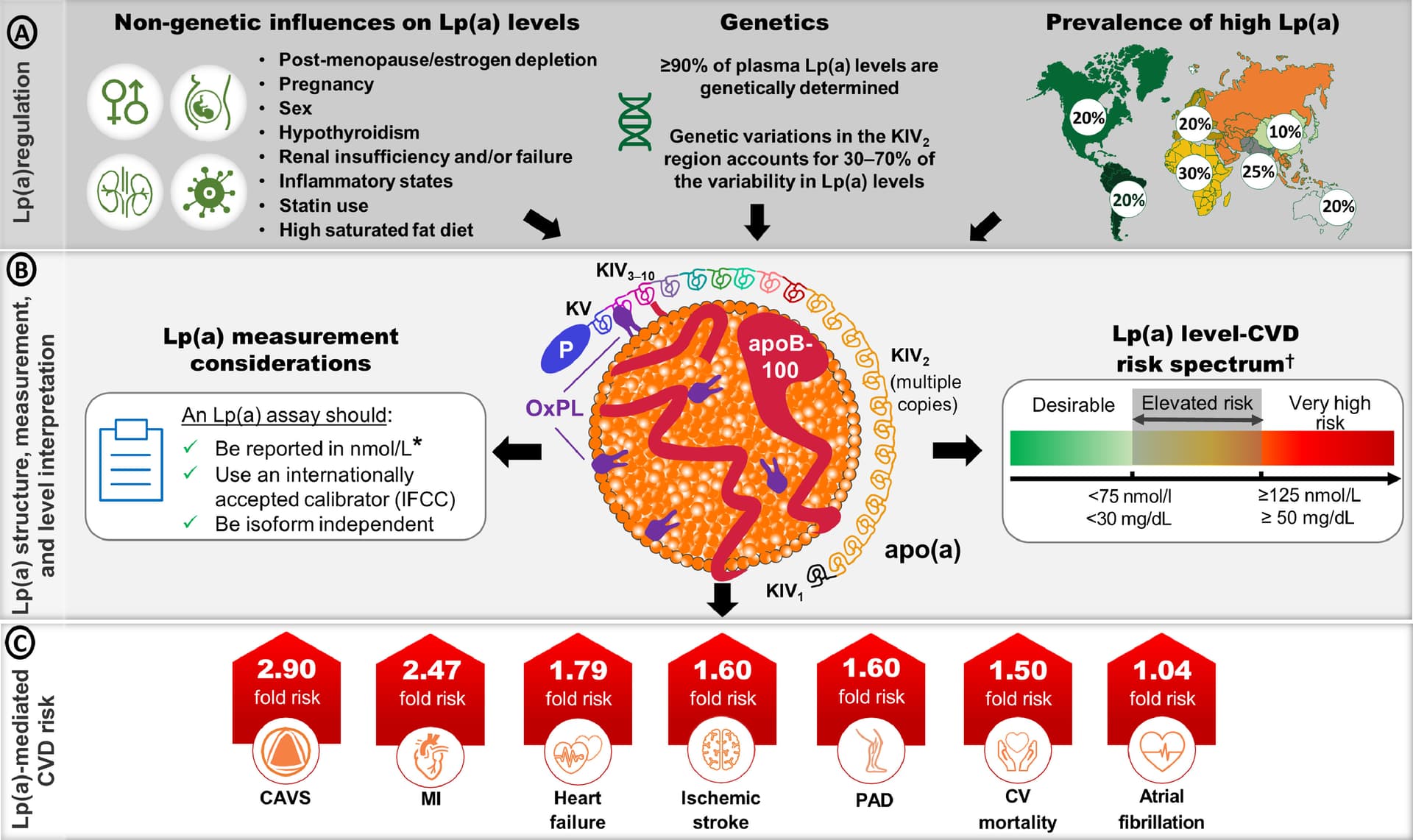
High Lipoprotein(a): Actionable Strategies for Risk Assessment and Mitigation 2024
Novel therapies that target apo(a) are at different clinical trial stages and substantially lower Lp(a) levels in patients with high Lp(a). This is critically important in the context of Lp(a) level population distribution, which is generally skewed, and has more than a 1000-fold range of concentrations between individuals. Therefore, those with the highest levels of Lp(a) will likely require large, absolute reductions in Lp(a) levels to effectively manage their CVD risk.
Two are in Phase 3: pelacarsen & olpasiran. We can expect approval in 2026 at best. Most likely 2027–2028.
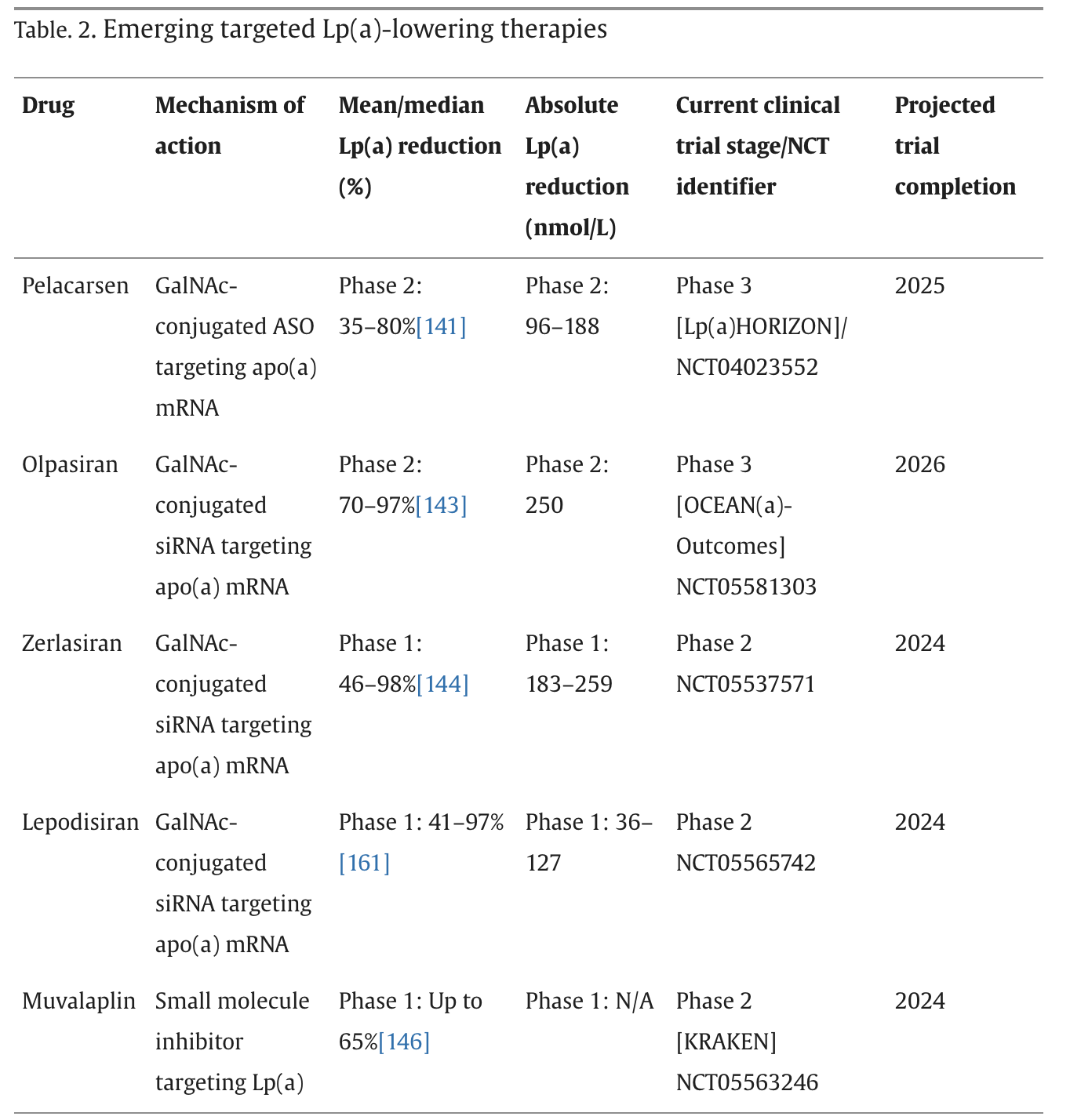
They also mention obicetrapib which divides Lip(a) by 2 (see also the dedicated topic: Obicetrapib (CETP inhibitor for dyslipidemia) - #48 by adssx ).
5 Likes
And then the challenge will be coverage/availability. Those of us with high Lp(a) but no history of actual cardiac events may not qualify for coverage for primary prevention. Hopefully it will be available from India ![]()
3 Likes
1 Like
Chris, can you give a one sentence intro or summary about the video - there are so many videos posted that most of us have to choose which ones to engage
And unlike links to papers or blogs, etc, one cannot “skim” a video to determine if one should invest in it or to just take away the high level.
Think it would be a great best practice for how we all can help each other in the most efficient and impactful ways.
3 Likes
FWIW: This is a short video.
3 Likes
It’s about 20 seconds long. For shorts, the summary is the title.
However, I could say short video at the top and you can read the title of the video.