I have questions about spiking and what is acceptable for good heart health, etc.
I just started wearing a cgm again, which I hadn’t done for a few months, and it does appear that my spikes are a lot higher again.
In general, I try to eat things that don’t spike my glucose too often because I seem to spike very easily (my first day wearing a cgm a couple years ago, I had Thai veggies, tofu and rice and went to 230-ish)
Since then, I started metformin. I rarely have oatmeal/regular pasta/bread/rice these days, and while I do have spikes, until starting rapa in March, by eating my restrictive diet and taking metformin, I most often have kept my spikes controlled in the 140-150 (not the case if I have anything I shouldn’t). But this has all changed.
I also started berberine last week.
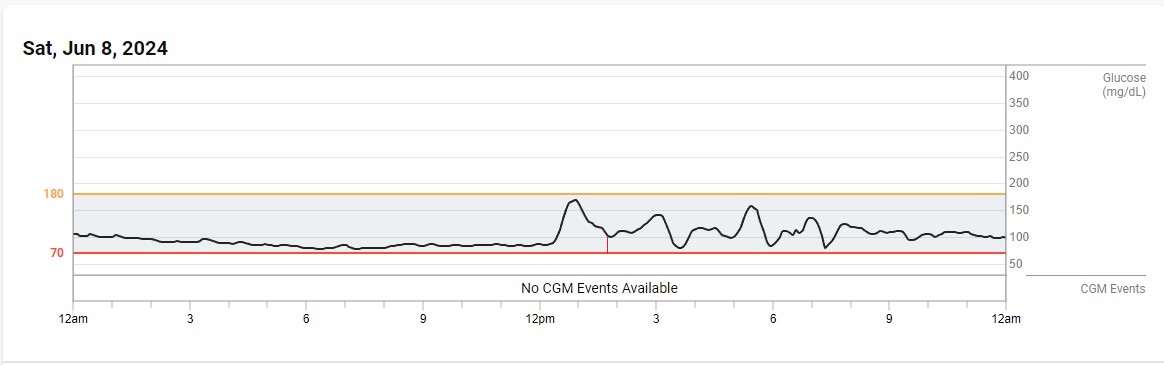
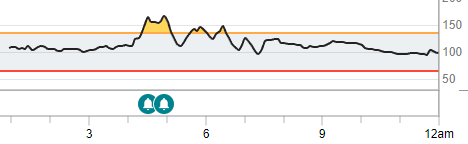
My spikes don’t last but I am going well above 150 quite frequently.
My question is:
In your opinion, what level of spikes are ok before you take action? (Additional drugs or even less ‘cheating’ with crazy things like healthy berries). Some say high spikes are fine if they come down quickly, but no one ever says what ‘high’ is… or how quickly ‘quick’ is.
And for a deeper dive… how many during the day, how long, what is a good baseline? I tend to eat between 6am-4pm, so I’m all over the place during that time, but from 6pm-6am, I’m mostly near 100-ish. (I can’t tell exactly because unless I just haven’t figured it out yet, you can’t go back and look at specific times and exact levels with the freestyle libre 3… you can easily get granular with the dexcom).
PS, I keep putting off my post rapa bloodwork because it involves a 40 minute drive and skipping my morning latte, so I’ve been lazy about it! I will do that in the next two weeks