Do you actually not believe in the relationship?
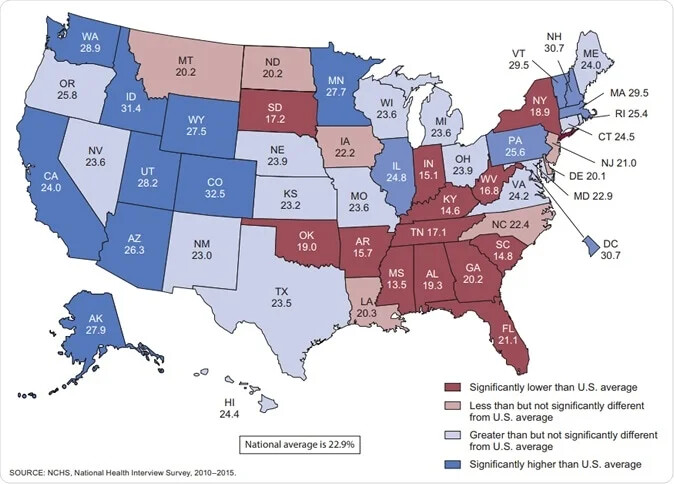
You can approximate the relationship by comparing US states with less vs more government support for health care and run the analysis within the 50 US states and will see the same picture.
Do you actually not believe in the relationship?
You can approximate the relationship by comparing US states with less vs more government support for health care and run the analysis within the 50 US states and will see the same picture.
I don’t know. I don’t have an opinion until I have data. Otherwise one could say with the same reasoning “Look, countries using the metric system have longer life expectancy!”
The US is so different in many ways than other wealthy countries that comparisons are hard. How do we account for the large immigrant population for instance? When you have thousands of poor immigrants coming in every year, it necessarily lowers the life expectancy. Does ethnic diversity also impact healthcare? Some drugs work better on some races (I have in mind CCB for black people), in an ethnically diverse country doctors have to deal with additional complexity. I assume in Japan the gene pool is less diverse and doctors are not confronted to that.
How do you measure “government support”? In Switzerland a lot of things are done privately but it’s well done compared to the stupid US system (especially the PBMs…).
More on Switzerland:
Switzerland has universal health care, regulated by the Swiss Federal Law on Health Insurance. There are no free state-provided health services, but private health insurance is compulsory for all persons residing in Switzerland (within three months of taking up residence or being born in the country).
The US after Obamacare is getting closer to the Swiss model if I understand correctly. And yet they’re way below in terms of life expectancy.
Perhaps this can shed some partial light:
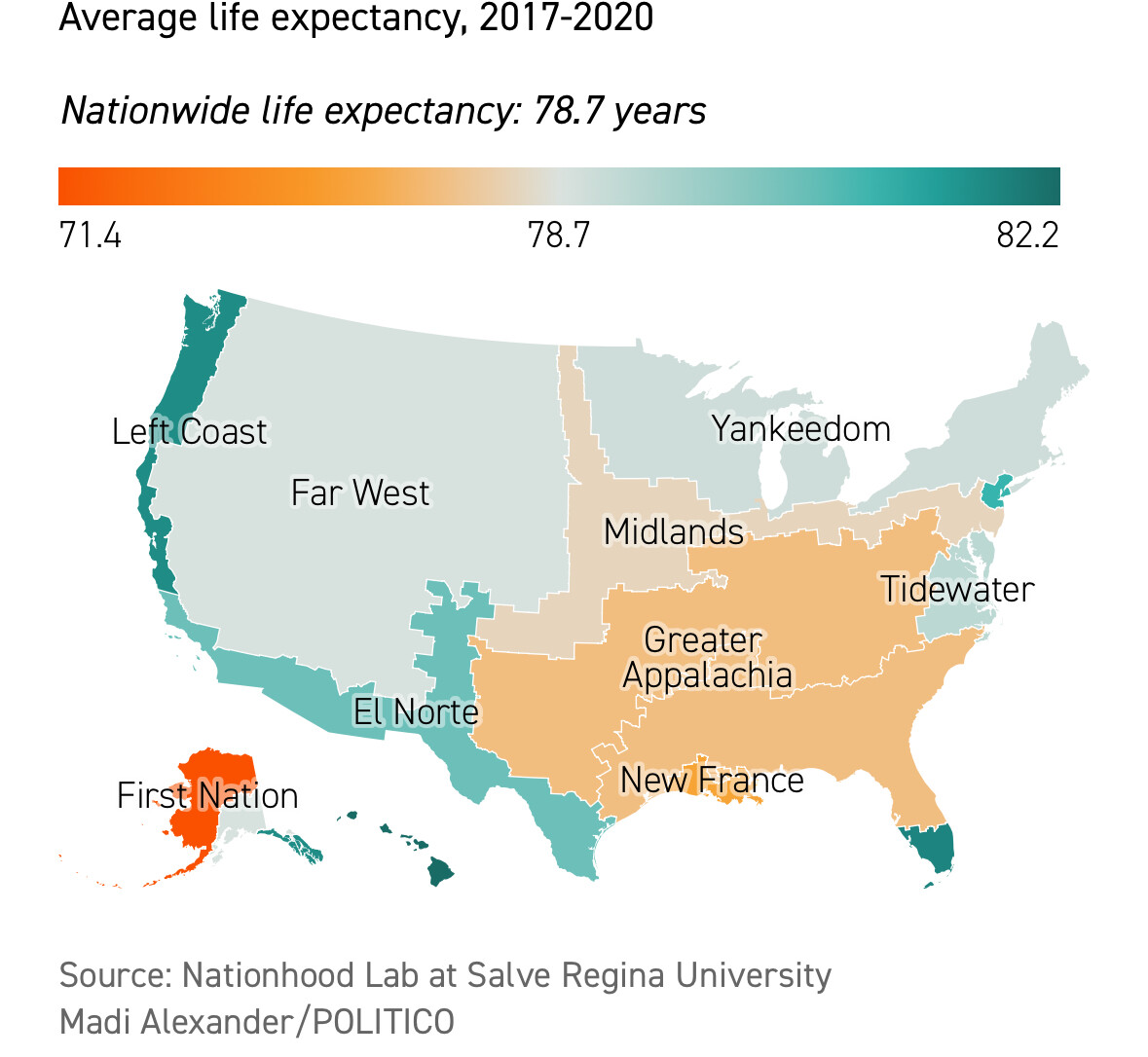
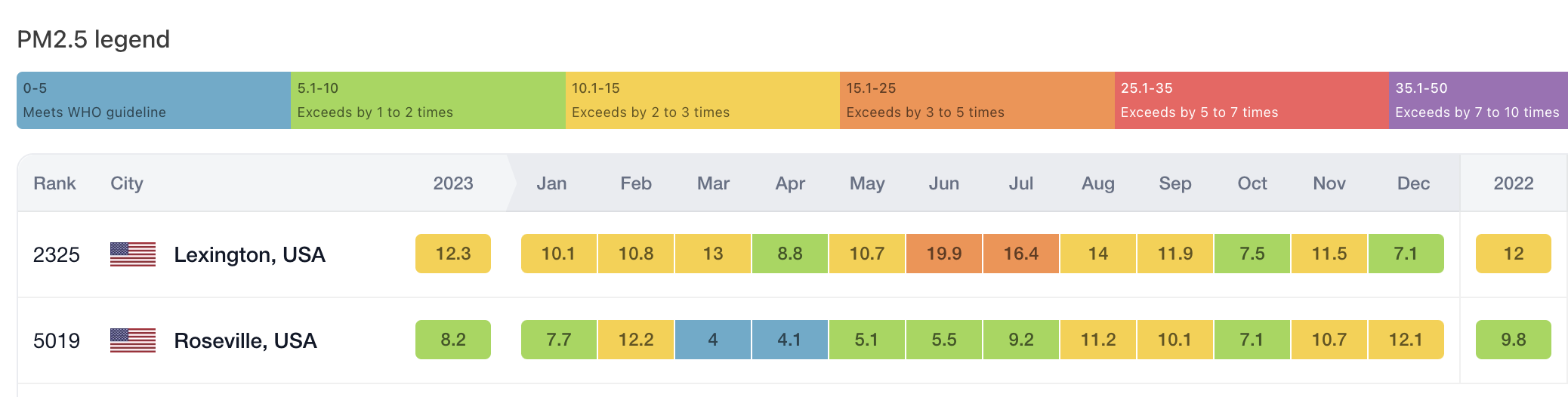
On paper, Lexington County, S.C., and Placer County, Calif., have a lot in common. They’re both big, wealthy, suburban counties with white supermajorities that border on their respective state’s capital cities. …But when it comes to how long their residents can count on living, the parallels fall apart. Placer has a Scandinavia-like life expectancy of 82.3 years. In Lexington, the figure is 77.7, a little worse than China’s.
Or take Maine’s far-flung Washington County, the poorest in New England where the per capita income is $27,437. The county is a hardscrabble swath of blueberry fields, forestland and fishing ports that was ravaged by the opioid epidemic and is almost completely white. It has one of the worst life expectancies in the entire Northeast: 75.5 years. But that’s more than six years better than the equally remote, forested, impoverished, white and drug-battered Perry County of eastern Kentucky.
So large are the regional gaps that the poorest set of counties in predominantly blue Yankee Northeast actually have higher life expectancies than the wealthiest ones in the Deep South. At a population level, a difference of five years is like the gap separating the U.S. from decidedly unwealthy Mongolia, Belarus or Libya, and six years gets you to impoverished El Salvador and Egypt.
The geography of U.S. life expectancy — and the policy environments that determine it — is the result of differences that are regional, cultural and political, with roots going back centuries to the people who arrived on the continent with totally different ideas about equality, the proper role of government, and the correct balance point between individual liberty and the common good
“We don’t have these differences in health outcomes because of individual behaviors, it’s related to the policy environments people are living in,” says Jeanne Ayers, who was Wisconsin’s top public health official during the Covid pandemic and is now executive director of Healthy Democracy Healthy People, a collaboration of 11 national public health agencies probing the links between political participation and health. “Your health is only 10 percent influenced by the medical environment and maybe 20 or 30 percent in behavioral choices. The social and political determinants of health are overwhelmingly what you’re seeing in these maps.”
https://www.politico.com/news/magazine/2023/09/01/america-life-expectancy-regions-00113369
I don’t think so - the Swiss system is probably better than many European systems in what actually level of healthcare universally actually is provided to its population, Obamacare is probably worse than most European systems in what universally actually is provided to people in the US.
The single figure of life expectancy at birth is useful, but does not separate out infant mortility and deaths as a consequence of accidents or violence.
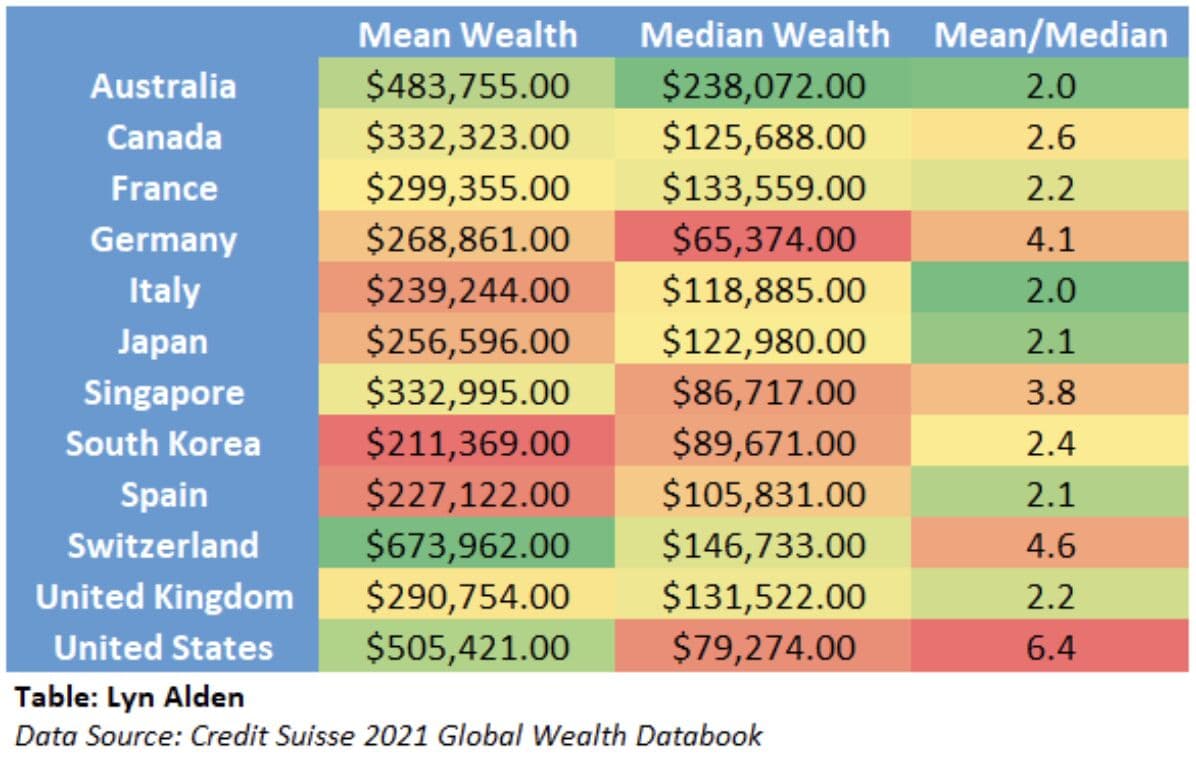
How does she conclude this? And what are “social” determinants of health? Wealth? Wealth inequalities are indeed so high in the US and wealth is a major factor for life expectancy (if not the main one?). The average American is 2x richer than the average Italian but the median Italian is 1.5x richer than the median American:
The above is independent of universal health coverage.
Looking at the example of Lexington County, S.C. vs Placer County, Calif.: if we adjust for individual behaviors, is there still a difference in life expectancy? For instance:
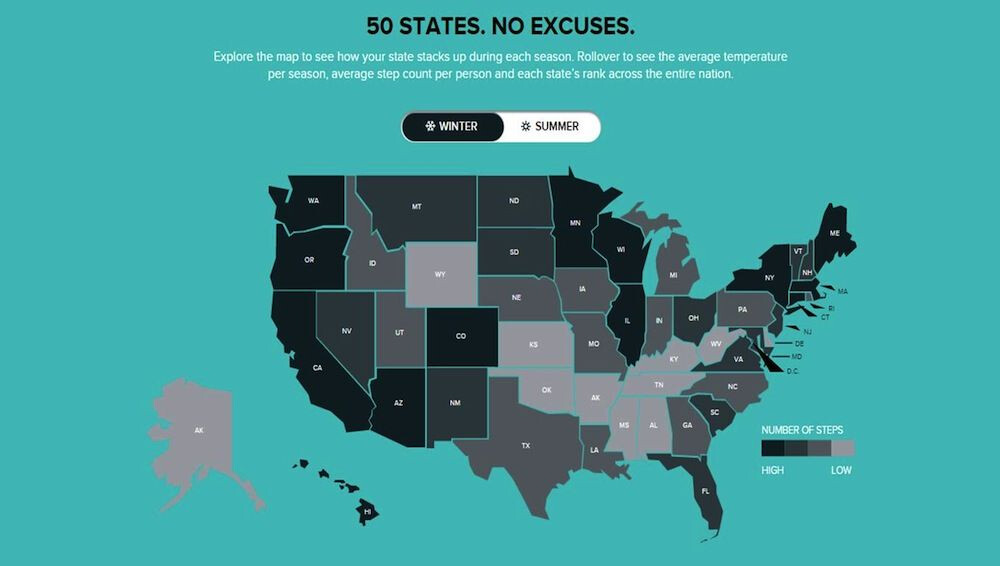
People walk more in CA than in SC:
SC is also significantly below the US average in terms of exercise, whereas CA is way above:
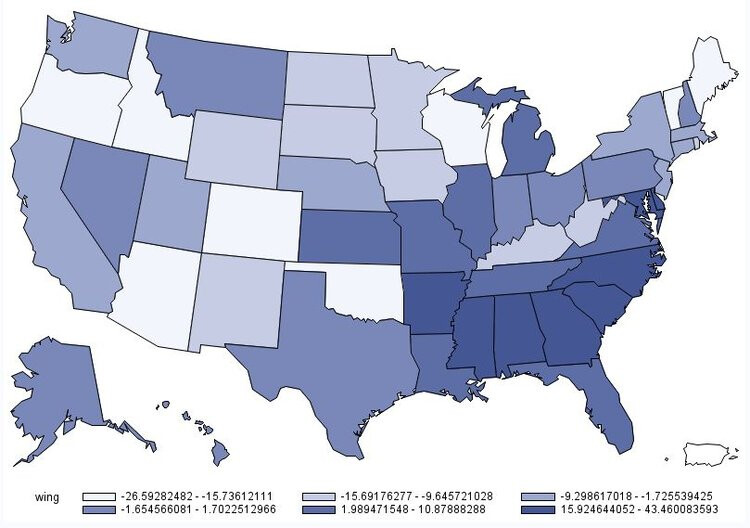
What about diet? South Carolinians eat way more red meat:
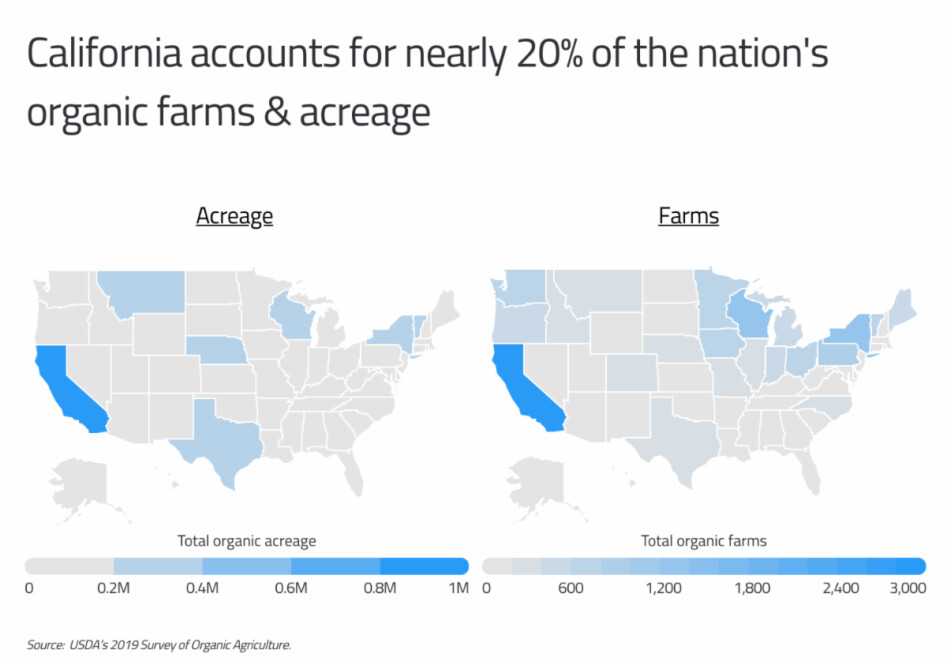
California is the top producer of organic food, so it’s way more available there:
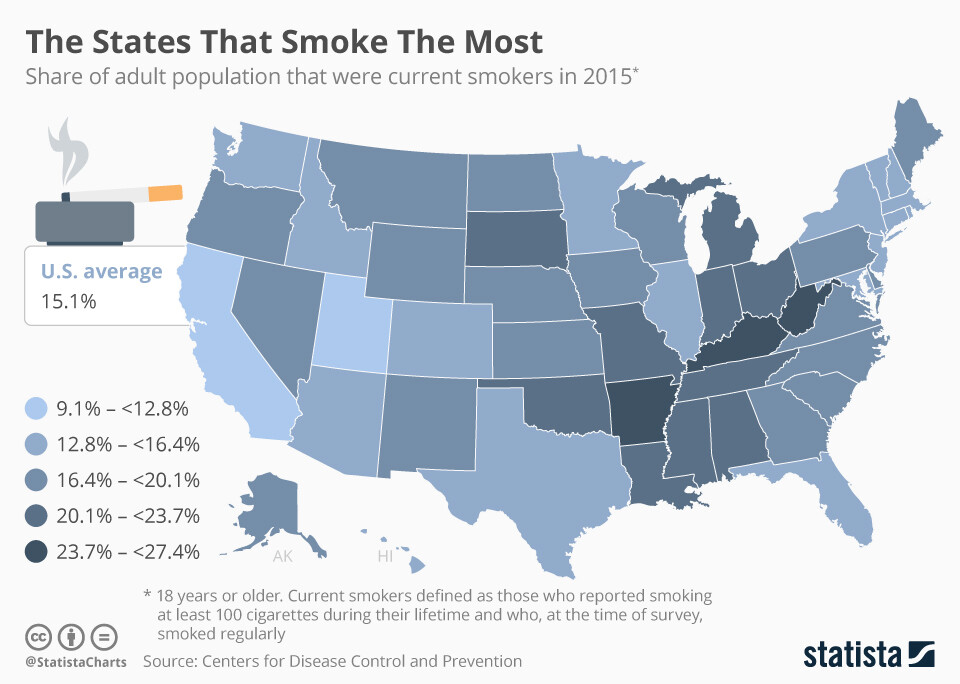
I don’t say that organic food is necessarily healthier, but it reflects that Californians are way more health-conscious. You can see this in their extremely low smoking prevalence as well:
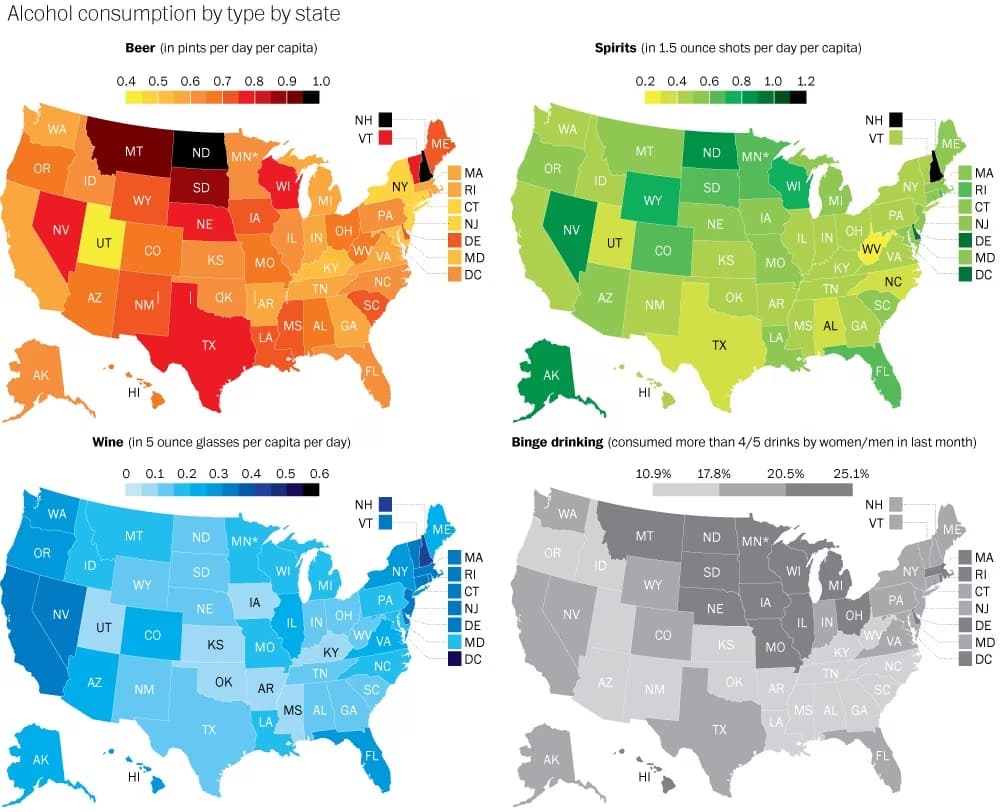
Californians drink wine, Carolinians drink beer:
The list goes on…
Similar differences exist between countries. So, do we have data at the global or national level explaining the contribution of different factors to life expectancy? Like diet (calories per day? organic %? % of processed food?), exercise (steps per day, exercise per week, sedentary %), wealth (average wealth/capita, median wealth/capita), medical environment (doctors/capita, hospitals/capita, etc.), health consciousness (like a questionnaire “How much do you care about your health?”, or the number of doctor consultations per capita per year), and then “universal healthcare coverage” (but is it just 0 or 1? How do you measure it? If the coverage is universal but provided by the private sector for instance?).
Of course, the US has the worst healthcare system in the (developed) world, and the Swiss one is among the best. I just said that in terms of concept (quasi-mandatory private healthcare coverage, 7.9% uninsured in the US as of 2023, 1.5–3% in Switzerland) they’re not that different since Obamacare. But the devil is in the details, and the way it’s implemented in the US is terrible.
Short video.
“Alzheimer’s […] you can find them out early and you can reverse them”
This guy is stupid.
I think he is arguing for prevention over treatments. As for Alzheimer’s, yeah he’s dead wrong. But for the others, it makes sense to detect early and prevent.
Jaye Rochon struggled to lose weight for years. But she felt as if a burden had lifted when she discovered YouTube influencers advocating “health at every size” — urging her to stop dieting and start listening to her “mental hunger.”
She stopped avoiding favorite foods such as cupcakes and Nutella. “They made me feel like I was safe eating whatever the hell I wanted,” said Rochon, 51, a video editor in Wausau, Wis. In two months, she regained 50 pounds. As her weight neared 300 pounds, she began to worry about her health.
I would not at all be surprised if all the warnings about “side effects” regarding GLP1 agonists were pushed by Big Food too.
I think it’s more because the US did not have a broad political consensus to go all in on real universal healthcare coverage (bad details and constrained execution was the compromise that was needed to get anything passed), while Switzerland and most of Europe and much of the OECD did have actual consensus for universal healthcare coverage.
Anyway, no need to spend more time on this on my end.