Yes this has been posted. I think the analysis is not as good as it should be - but appreciate their methods.
I’d go Rapamycin, SGLT2’s/GLPs - can’t pick a winner there, and they miss telmisartan, PDE5’s.
I don’t see their basis for adding Bisphosphonates. Metformin fine in diabetics - but otherwise doesn’t have evidence. Aspirin doesn’t improve longevity except in high risk individuals. I’ll take amlodipine over most beta blockers - and isn’t mentioned.
Like the acarbose and methylene blue.
Dasatinib/Quercetin/Fisetin is an interesting area. I have mixed evidence on this and have a few patients doing this q3 months.
Discussed here: New Paper: Summary of the top FDA-approved Drugs that can be Repurposed as Gerotherapeutics / Geroprotectors - #2 by RapAdmin
And I agree with @DrFraser, as usual! (Beta-blockers are also not a homogenous class)
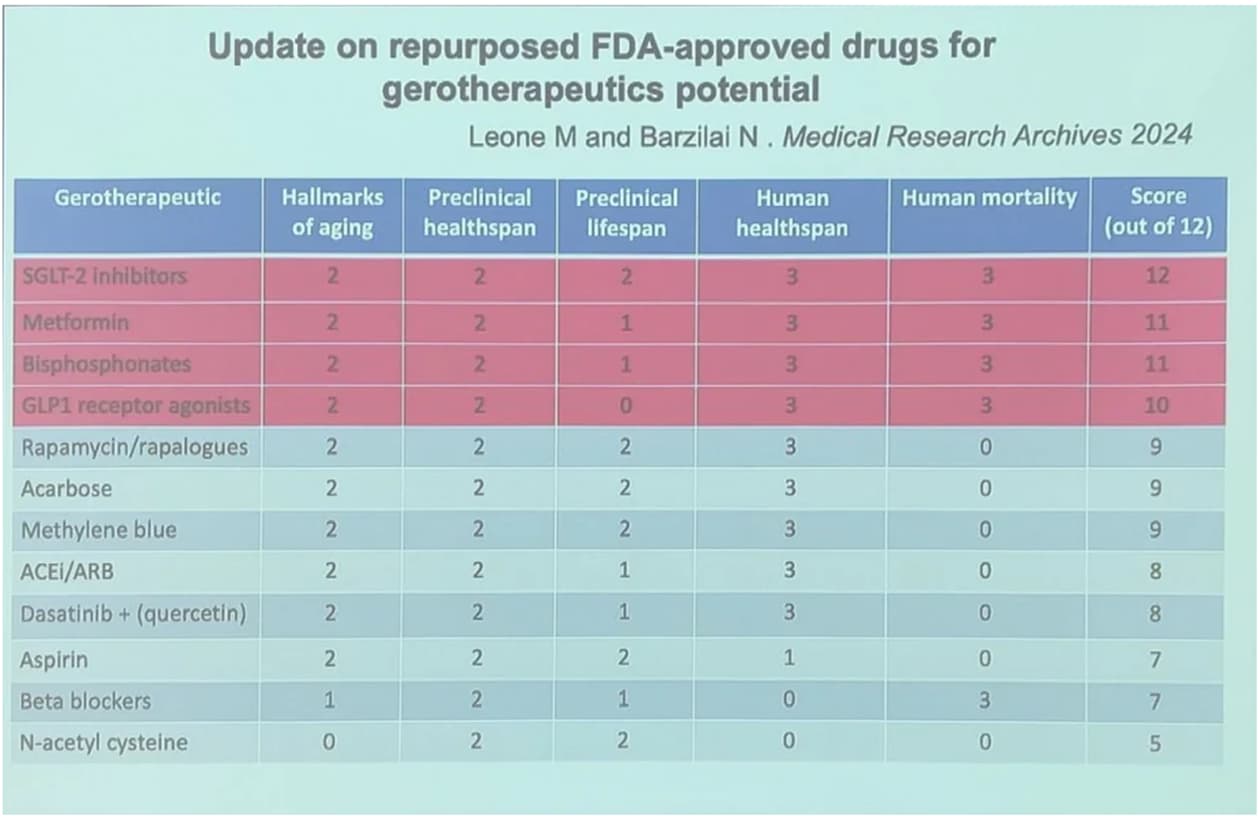
Am I to read this that supposedly SGLT2’s are better than say Rapa for longevity (12 vs 9 score)? In other words, the best thing that one can do for longevity is to take anti diabetes drugs? Interesting and would def agree for diabetics and perhaps preD’s but is there enough evidence to say that it has same benefits for non-diabetics?
It’s not an either or - they are lovely partners along with a GLP-1 and lipid management.
It should always be a package deal … do things to maximize insulin sensitivity, especially in the brain, optimize lipids and then take Rapamycin which makes those things slightly worse on average, but medicated you have much better numbers.
If I had to pick 5 things to do (outside of lifestyle/exercise/diet) it would be Rapa, GLP1, SGLT2, Lipid management, blood pressure management. These have roll on effects to other causes of death and disability such as Neurocognitive decline, sarcopenia, malignancy … and naturally improve risk of stroke/heart attack/vascular disease.
The most critical thing is don’t take Rapamycin to fix everything - it won’t. Optimize everything and have Rapamycin as part of the package.
As usual - talk with your “PCP” before doing anything.
Thanks DrFrazer, great info.
One question on these two points though “Lipid management, blood pressure management”. Assuming one has these at normal levels is there any evidence (to your knowledge) that using such meds has any benefit on perfectly healthy individuals, as an example. There seems to be data (even if not conclusive) that some of anti-diabetic meds may extend their benefits to other functions/organs, yet not sure if Lipid and pressure management meds would have some or same benefits?
Their scoring rubric is reported below. While the criteria and cutoff points for each scoring point allow for a certain amount of intersubjectivity (I assume it was a team effort) this is not necessarily bad. The rubric might have been more rigorous had scoring consisted of blind panels with concordance rating. Still, it is a decent method. To quarrel with their rankings would correctly involve quarreling with the conceptual and empirical bases for their criteria not with a particular purported geroprotective unless its material facts in application have been misrepresented. Their scaling however does impose some compression (nonlinearity) on some ratings. I’m not sure why they made that decision.
Based upon new drugs included in Drug Age, a database for drugs that extend animal lifespan, evidence from a review of the literature, and discussions with experts in the field, we identified three new drug classes with acceptable safety profiles to be included in this update: GLP-1 receptor agonists (GLP1 RA), beta-blockers, and bisphosphonates. As our prioritization only has FDA-approved drugs, nutraceuticals and supplements were excluded. Our review of the preclinical and clinical evidence for each drug followed the same protocol outlined in the original paper. Preclinical categories included rodent lifespan, rodent healthspan, and hallmarks of aging. Clinical categories included human mortality and healthspan. Our scoring for each category was also the same as the prior paper, allotting a maximum of 6 points for preclinical evidence and 6 points for clinical evidence for a maximum of 12 points total. Preclinical points were allotted using the following: (i) rodent lifespan: 0 points for no effect on lifespan or no applicable studies, 1 point for lifespan tested outside ITP, 2 points assigned for a significant increase in lifespan within ITP; (ii) rodent healthspan: 0 points for no effect on healthspan parameters or no applicable studies, 2 points for a positive effect on healthspan; (iii) hallmarks of aging: 0 points for no hallmarks, 1 point for one or two hallmarks, 2 points for three or more hallmarks.
Clinical points were allotted using the following: (i) human mortality: drug needed to demonstrate that it reduced all-cause mortality or death from a disease which it was not intended to treat, with 0 points for no applicable studies or negative findings, 1 point assigned for observational studies, and 3 points assigned for RCTs; (ii) human healthspan: drug needed to demonstrate that it targeted at least one age-related disease/pathologic process which it was not intended to treat, with 0 points for no applicable studies or negative findings, 1 point assigned for observational studies, and 3 points for interventional RCTs. In addition, drugs with evidence supporting improved mortality from COVID-19 were distinguished with an asterisk in Table 1.
@RobTuck Nice analysis and in line with my views. I admire your intellect. The issue is the lack of trials with Rapamycin and the over valuation of metformin in non-diabetics.
@RapMet The questions you ask are really sensible and ones I answer multiple times daily. So if someone’s blood pressure can safely be lowered by 10-12 mmHg (Systolic) I’d like to get someone on 80 mg of Telmisartan. If someone doesn’t have an absurdly low ApoB/Lp(a) then I’d like to do something to optimize that.
The evidence in the literature really needs to contextualized. It is for fixed durations, not in patients like most of us, and not in people goaling for 100+ years of quality life. The short term outcomes aren’t of much interest as they don’t represent drug efficacy with BP/Insulin Sensitivity/Lipids … instead they are confounded by pre-existing disease. The long term outcomes are what we have so much less information on and is the relevant discussion.
I have no vascular disease … and I want to stay that way – for the next 50 years … how do I accomplish this? What study answers this question?
I also ask this, as I feel quite healthy and I’m not crazy about taking pharmaceuticals. My blood pressure is 110/73 and my HbA1c is 5.1, are you saying I should take pharmaceuticals anyway because of their longevity benefit? I’m convinced on rapamycin - and combining it with metformin/acarbose because the concept of slowing down your overall metabolism when you get older makes sense to me. I already have just naturally started eating less (even though I love food) because this is what my body is telling me. I don’t want to lose weight or eat less - if anything, I need to make sure to get enough protein for muscles. I am taking atorvastatin (10mg) and ezetimibe (5mg) not because my ApoB was particularly high (87) but because my Lp(a) was (195nmol/L). Although the statin side effects are minor and won’t make me stop, I don’t feel as healthy as I did before starting them (less desire to lift weights). The optimum for me would be to take no pharmaceuticals and I feel like I would make it to 100 just on lifestyle alone. But with Rapa…120. I’m thinking about imaging (CAC and/or CIMT) for plaque and if I could keep it at Zero or very low, I would stop lipid lowering drugs, too. For me imaging trumps ApoB and if I knew that I didn’t have a plaque problem, and I kept watching it, I’d stop caring about ApoB. The interventions on the horizon that look good are IL-11 inhibitors and partial cell reprogramming because they are more system wide. And of course the little things like mental sharpness and sharpness of all the 5 senses could always be better. And energy, motivation, productivity, creativity…who wouldn’t want more of those? But otherwise, I’m good…and happy with life. I don’t want to be a walking Pharmacy. It baffles me why people here are so drug happy. I guess science is the new religion…we can’t trust anything else, so let’s put all our faith in science - to part the waters and lead us to the promised land. I’m old school and still worship nature…I’m thinking of joining the Shinto religion and moving to Japan (maybe I’ll just watch Japanese movies).
Thanks again and great info.
Obviously no medical advice is being sought on here, but if I’m reading and understanding it correctly you seem to be of the opinion that using certain meds as a precaution against vascular/heart disease may not be such a bad idea even if the indicators are within normal range? If that is so I tend to agree (we all probably heard of cases where someone had a heart attack out of nowhere, that otherwise they seemed perfectly healthy) but perhaps at much lower doses than one would take if they were in high-risk category. If I experiment with some drug (not because of a certain condition I might have) I always tend to keep dosage within 10- 20% of the lowest recommended dose. My thinking is that such low dose minimizes the adverse effects and still might provide some maintenance/precaution benefit.
It might be me, but I tend to be scared to take a full recommended dosage of something that I do not need (other than RAPA that is). Or is it the case (for most meds, including CVD ones) in which unless you take the minimum recommended dose, anything less might be futile? And I’m afraid that this is another question for which there is no definite answer, but I’ll ask anyway ![]()
Standard lipid advice here is yes, low dose statin, usually 10mg atorvastatin or 5mg rosuvastatin with 5mg ezetimibe. Then keep testing to reach target range for ApoB - 60-70 for normal optimum and 60-50 or less for extra safe. Have you done any imaging to check for existing plaque levels? How old are you? How good is your metabolic health - HbA1c, Hs-CRP, BMI, blood pressure, as well as the ApoB and fasting blood glucose (HOMA-IR for insulin resistance, even better)?
The life extender (drug) with the best track record so far is rapamycin and combined with metformin and/or acarbose even better. I think the evidence for metformin, so far, exceeds that of SLGT2 or GLP1 - if you are already lean - for lifespan and healthspan (even for non-prediabetic) @DrFraser may disagree. My experience on 850 mg of metformin/day is no effect on exercise/muscle building, whereas statins were a negative…but everyone is different. Bempedoic acid might be the answer and I’ll try that on my next order to India.
**That’s my opinion anyway, and I have no credentials. Let’s see what the doc has to say.
You have a great intellect … don’t need letters after your name.
So the issue of being “healthy” and taking medications is a interesting concept.
I don’t look at necessity, I look at risk/benefit.
So if you have adverse effects with statins … don’t take them. Also, if you’re worried about vascular disease, measure and see do you have some. If not … chill out … if yes, then seriously risk mitigate and monitor closely.
I take a multiple medications despite having no typical medical indication for doing so … but do I want the typical outcome with typical care of dying as a man at 76 years old in the U.S. or do I have very different goals?
This is where the guidelines and the typical studies really fail to answer this question.
The studies can give us an idea on risk mitigation … and I think we mitigate risk at mid life or earlier onward.
HOMA-IR is great for peripheral insulin resistance, but doesn’t tell us about the brain … it looks like much of neurocognitive decline relates to brain insulin resistance … taking things like GLP1’s/SGLT2-i are worthy of investigation and consideration.
Hopefully my perspective on this is helpful.
@RapMet On the CAD side of things … measure if you have disease … don’t take an ApoB/Lp(a)/HsCRP as sufficient reassurance. No one wants their first awareness they have vascular disease to be death or disability. Don’t be falsely reassured by protocol driven medicine - which is for the masses - but if interesting in not ending up dead or disabled, get a CT Calcium+Carotid Intimal Media Thickness ultrasound or a whole body MRI with MRA neck/head like Simonone does. Either strategy is a useful addition to blood work … but if someone has measurable disease it’s progression is unpredictable and aggressive treatment is my general approach.
Hopefully that helps clarify.
Very clear and thank you.
I’d say that’s pretty good for a no credentials guy…Thanks for the info/advice.
What are the criteria for scoring? Have the paper being peer reviewed?
Of course, I agree and I love to hear your perspective. Like most everyone here, I try to look at my own individual health case and circumstance and then apply the wisdom I learn here to my own situation. I feel confident reading and in-tune with my own body - no, I can’t guess my plaque levels but I don’t think they’re terrible…knock on wood. Certainly, I do extensive reading online to try and determine what is the best preventative before any indication of a problem but the research often isn’t conclusive so you have to rely on your best judgement. And the brain is still a bit of a mystery although new discoveries and research are now moving at a rapid pace, it’s one of my primary focuses. I’m open minded on SLGT2 and GLP1 because glucose/insulin, inflammation and circulation and the gut microbiome are key factors. I think metformin looks good, too. The new research on IDO1 looks very promising. “Recent research has implicated an enzyme in astrocytes, called indoleamine-2,3-dioxygenase 1 (IDO1).” Cardiovascular and brain health are at the top of my agenda…cancer, I’m just hoping for a little luck…Simonone looks good, I’m high on imaging…just wish it were cheaper. I’m doing blood tests every 3 months with many add-ons to the standard panels. I think that’s the most useful thing you can do for lifespan/healthspan, at least until a better BioAge clock test comes along.
I’d skip the blood work for a year and grab a Simon Scan. Yes a wallet biopsy - I’ve only done it once, but well worth it, very valuable information which can change health decisions, so long as you don’t start investigating “incidentalomas” which are not of any significance. Neither my wife or I had anything abnl (except she has a much better developed hippocampus … which might explain my record of losing arguments with her!) which was a surprise.
The blood work isn’t that helpful comparatively … especially not every 3 months … how many action points do we get from this? Knowing if you have vascular disease (or some little area of malignancy) is pretty valuable, and the bloods often won’t answer that question — actually worse than this, “normal” results reassure people that everything is fine, when it isn’t.
What!!! That should set off the red light flashing in @RapAdmin office. Blasphemy! For biohackers that’s like the “holy grail”… @John_Hemming gets them weekly (just to make the rest of us feel bad). Yes, I want to get a Simon Scan (and I still haven’t gotten my VO2 Max test) but I’d sell one of my children before giving up my blood tests…oh, wait, I don’t have children…well, maybe my motorcycle. Trying to tweak your blood tests with micro-adjustments in lifestyle and supplements is what we live for…just ask Michael Lustgarten @ConquerAging . I think I’d become suicidal.
what a waste of his/someone’s/taxpayer’s money. I’ll stick with every 12-18 months.
You better be careful…he’s one of the elders here…and we respect our elders. Not like you young whipper-snappers…the world’s going to hell, isn’t it?