Thanks, but I’ve had multiple URIs (Upper Respiratory Infections - COVID or flu) not UTIs (Urinary Tract Infections). I’m not aware of SGLT2Is affecting URIs?
1 Like
Oh, I misread what you said then. It seems it should be called URTI, by the way, maybe because people like me can misread it ![]()
No, for URTI it should be fine.
1 Like
Yes, URIs are also known as URTIs. ![]()
More SGLT2 ads @DeStrider! ![]()
Sodium-glucose cotransporter 2 (SGLT2) inhibitors reduce the risk of cardiovascular disease in patients with chronic kidney disease (CKD) or heart failure, with similar relative effects in people with or without type 2 diabetes.
Overall, SGLT2 inhibitors reduced the risk of cardiovascular death by 20% (HR 0.80, 95% CI 0.68 to 0.95, N=523 deaths), with consistent effects across the trials. Relative risk reductions for fatal heart failure (HR 0.41, 95% CI 0.23 to 0.72, N=64 deaths) appeared more pronounced than other causes of cardiovascular death (HR 0.88, 95% CI 0.73 to 1.06, N=454 deaths)
While many hypotheses have been suggested to explain the large reductions in heart failure observed with SGLT2 inhibitors, precise underlying mechanisms remain incompletely understood. Multiple mechanisms may contribute, including augmented natriuresis and reduced volume overload, anti-inflammatory effects, and potentially direct effects on myocardial energetics. It is possible that the effect of SGLT2 inhibitors on proximate causes of cardiovascular death differs across populations. For instance, in patients with heart failure, SGLT2 inhibitors appear to reduce the risk of sudden cardiac death.
Efficacy of Sodium-Glucose Cotransporter 2 Inhibitors in Patients with Acute Coronary Syndrome 2024
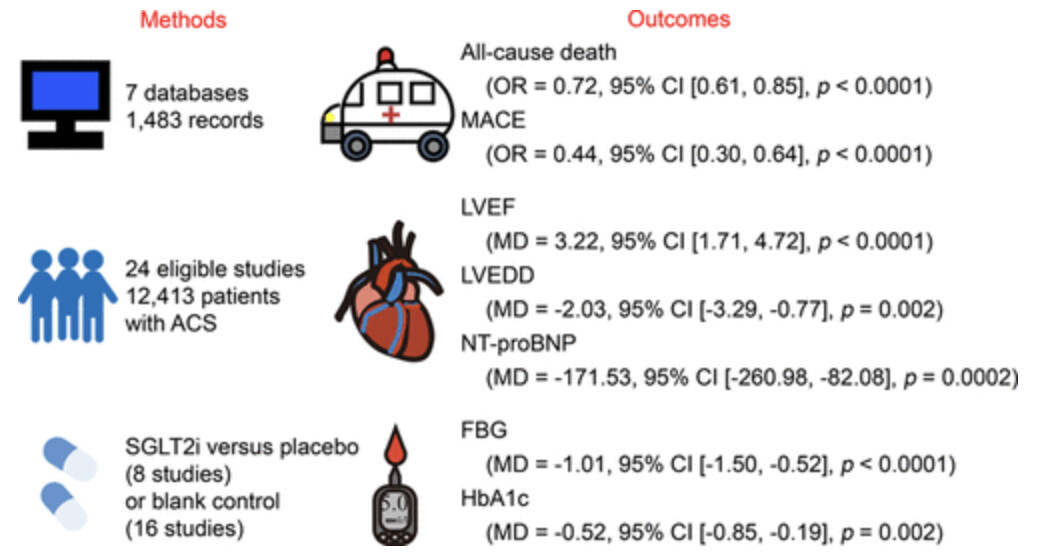
(looks like the authors asked their kids to illustrate the paper ![]() )
)
4 Likes
What is a meaningful combination strategy for using SGLT2-inhibitors (empagliflozin) alongside acarbose (reducing glucose peaks), berberine (amplifying AMPK at cardio-days), and metformin (synergetic around rapamycin days)?
Any thoughts on this?
1 Like
Metformin and Empagliflozin together achieve better results for lowering HBA1C than taking either alone. Most T2D patients take both. Acarbose reduces glucose spikes. Berberine is a Metformin substitute (almost). The way to tell if you are doing to much is if you experience bouts of hypoglycemia. You may need a glucose monitor to detect if your glucose levels get too low.
Metformin can give you hypoglycemia. I have read that Empagliflozin will not. Acarbose will just give you gas. ![]()
3 Likes
No:
- Canagliflozin - Another Top Anti-aging Drug - #658 by adssx (see the illustration)
- See also: Metformin and Canagliflozin Are Equally Renoprotective in Diabetic Kidney Disease but Have No Synergistic Effect 2023
- Antidiabetic medication and risk of dementia in patients with type 2 diabetes: a nested case–control study 2019: “Analyses of the most frequent treatment regimes did not show any synergistic effects of combined treatment.” (I don’t have the full text but I think it was mostly about metformin + SGLT2, as GLP-1 + SGLT2 probably have synergies)
1 Like
Speaking of synergy, does anyone have experience with SGLT2 and DPP4 inhibitor combinations? I am considering Glyxambi (Empagliflozin/linagliptin) specifically.
Several diabetic courses include an SGLT2I and Metformin combined into one pill as a course of treatment. Here’s a source from the Mayo Clinic:
Empagliflozin And Metformin (Oral Route) Description and Brand Names - Mayo Clinic.
The combo medicine’s name is SYNJARDY.
In addition, my mother’s cardiologist prescribed Metformin and Empagliflozin. There must be a synergy otherwise they wouldn’t be prescribed to treat T2D.
See also:
The clinical data reviewed show that the combination of empagliflozin/metformin offers the potential to improve glycemic control in T2DM and reduces body weight and blood pressure, vs each agent individually,
At week 24, adjusted mean reductions in HbA1c from baseline were significantly greater for patients receiving empagliflozin/metformin twice daily than those receiving either empagliflozin once daily (P < .001) or metformin twice daily (P < .01). Significantly greater proportions of patients treated with combination therapy reached HbA1c <7.0% at week 24 compared with patients who received either agent alone (P < .05 for all comparisons).
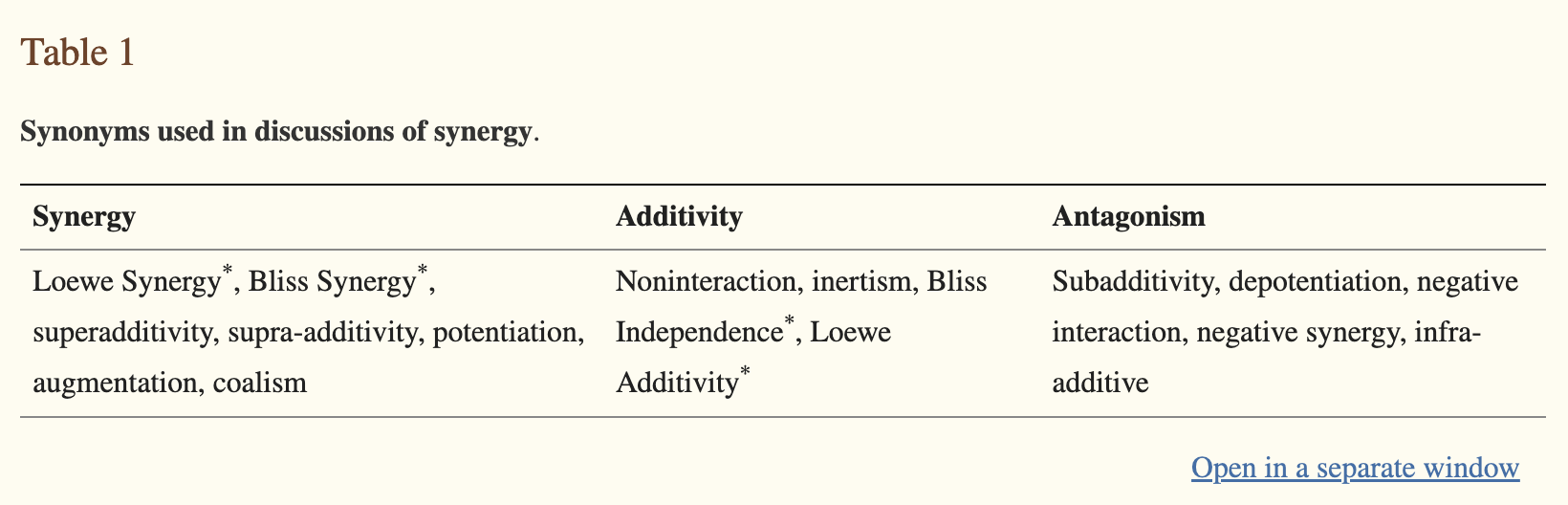
Synergistic means that the combination produces “a combined effect greater than the sum of their separate effects”
This is not the case of metformin + SGLT2. In terms of long-term outcome, the data I found (posted above) shows that metformin + SGLT2 does not do significantly better than metformin alone.
The paper you cited cites this study: Initial Combination of Empagliflozin and Metformin in Patients With Type 2 Diabetes 2016
They found the following reductions in HbA1c:
- Empa + metformin: −1.9 to −2.1% (depending on the dose)
- Empagliflozin alone: −1.4%
- Metformin alone: −1.2 to −1.8% (depending on the dose)
So we have:
- −1.2 + −1.4 = −2.6 < −1.9
- −1.8 + −1.4 = −3.2 < −2.1
Empagliflozin and metformin are, therefore, “subadditive”, so there’s no synergy (it’s even worse as the expected outcome is often additivity).
4 Likes
Gliptins are not cardioprotective. It’s not clear if they’re significantly better than metformin. They might be neuroprotective though: Are dipeptidyl peptidase 4 (DPP-4) inhibitors [like sitagliptin and Linagliptin] similar at all to semaglutide? Do they reduce appetite/are they ever worth it?
My guess is that GLP-1RAs are better than DPP-4i and that the best combination is GLP1-RA + SGLT2i. But it’s nothing more than an assumption.
2 Likes
Yes, they may be subadditive, but taking both substances reduces HBA1C more than either one alone. So, yes, I guess they are not synergistic. However, when you are treating T2D, you are trying to get HBA1C back to normal ASAP.
I would argue that the majority of interventions we initiate for longevity are subadditive as well. However, that doesn’t mean it isn’t in our best interest to get whatever extra effects for lifespan or healthspan we can.
1 Like
Yes, for sure. I only commented on metformin and SGLT2 not having synergy (actually, the opposite: there’s a negative interaction).
Then, is metformin itself good, that’s another question.
2 Likes
Highly unlikely IMO.
I have been using metformin for decades and have experimented with various dosing levels and have never experienced dangerously low blood glucose levels. Maybe people who have type II diabetes react differently to metformin.
1 Like
Does anyone see a “conflict of interest” between metformin and Jardiance? Would it be unhealthy to use both?
The times when I have experienced hypoglycemia has been while taking a relatively high dosage of Metformin (1.5-2 g daily). I would get hit with hypoglycemia at around 4 pm on regular occasions. It feels like a heart attack but goes away in a few minutes if you take sugar. If I don’t take high levels of Metformin, I don’t experience the issue.
My doctor told me it was hypoglycemia, so that’s what I have assumed.
2 Likes
I think you mean drug interaction. It’s used in a combination pill. Metformin isn’t that good though, except for those it is indicated of course…?
1 Like
Well, actually I am looking more for “is there any synergies” or they both work on their own way. I tend to say things not so directly from time to time. Anyway, As far as interaction I don’t think there any interaction. Since we are on the subject does acarbose makes sense to be taken in addition to Jardiance?
See this thread for a past discussion on this question: Combination of Rapamycin, Acarbose, and SGLT-2 inhibitor
3 Likes
I eat four meals per day. I take 10mg Empagliflozin with breakfast, then 50mg Acarbose with each of the following three meals (150mg total). I would imagine it’s synergistic. I believe they are prescribed together sometimes.
3 Likes