For the reasons @adssx mentioned, I’d think about pushing the dose of telmisartan gradually to 160 mg with monitoring if needed to get into a good BP range. If that ends up being inadequate, you’ll have great PPAR effects, and a tiny dose of a third agent could be considered, or a different CCB that doesn’t risk edema, in a higher dose could be considered.
2 Likes
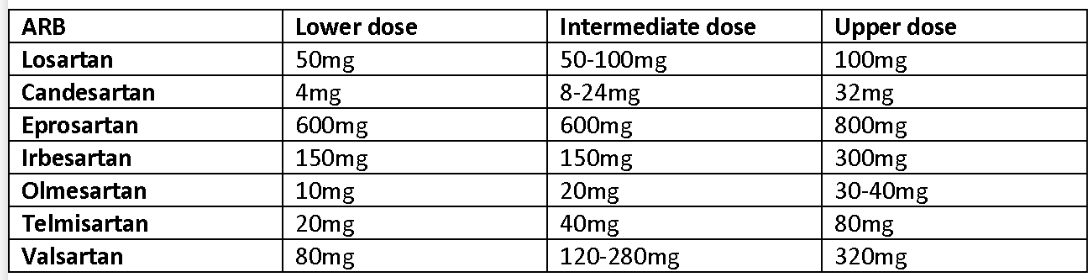
Not really. But my mom was on 40 mg Telmisartan while switched from other ARB equivalent (50mg Losartan) but at the end she had to double it to 80mg by her doctors because its “weak action”. Here is the equivalency chart:
Why do you think indapamide didn’t help you? Any sides?
I wouldn’t take high doses of telmisartan just to extend longevity or to possibly ward off dementia in the vague and distant future. But that’s just me.
I did order some hawthorn though. I think it’s worth an experiment.
Her doctors are stupid. Make sure to change doctors.
These equivalency charts are just a help. They say nothing about the potency of a drug. What matters is the effect on biomarkers (here SBP, DBP, PP, MAP, BPV, HOMA-IR, etc.).
3 Likes
I felt quite bad taking it (only 2 weeks). But I had issues with my glucose variability before and thiazides can mess up glucose regulation in some people. So I’m just unlucky to be one of those.
Anyway I’m on telmisartan 80 mg + amlodipine 5 mg + dapagliflozin 10 mg + taurine 3 mg and still have elevated BP ![]() I’ll discuss Hawthorn and COQ10 with my doctor…
I’ll discuss Hawthorn and COQ10 with my doctor…
4 Likes
You can do a deep dive on Carvedilol ( beta blocker seems to be superior to nebivelol ) or Nifedipine a calcium channel blockers with positive effects on elastin and utilize one of them or both.
1 Like
I start the day with hibiscus tea. This is also thought to help lower BP.
I buy the dried flowers by the kilogram from healthysupplies.co.uk
1 Like
Tim, why not add an SGLTi like dapa or empagliflozin? You’d get all the potential health benefits along with at least some additional drop of BP.
2 Likes
Thanks for the recommendation. Yes, these meds sound attractive but the potential sides give me pause:
“The main adverse events of SGLT2i include urinary tract and genital infections, as well as euglycemic diabetic ketoacidosis. Concerns have also been raised about the association of SGLT2i with lower limb amputations, Fournier gangrene, risk of bone fractures, female breast cancer, male bladder cancer, orthostatic hypotension, and acute kidney injury.”
Now this may be a lawyer talking, doing a nice job of CYA. Plus, I don’t have diabetes, so most of the warnings probably don’t apply to me. I’ll talk to one of my docs about it. It could be just the thing.
2 Likes
That’s the position I’m taking for myself – that the scary sounding side effects are not only extremely rare, but even more extremely rare in a non-diabetic. If you haven’t read through the thread titled “Canagliflozin – another top anti-aging drug”, the published studies on the safety of these meds are very reassuring to me, and the potential health benefits appear to be enormous.
4 Likes
Last time I checked nifedipine it was inferior to amlodipine. And its 2h half-life is way too short to ensure good BP control over 24h. Carvedilol is interesting but I think it lowers heart rate and mine is already in the lower range of normal.
Hibiscus tea: interesting but not convenient when traveling.
3 Likes
Telmisartan Reduces LPS-Mediated Inflammation and Induces Autophagy of Microglia 2024
We conclude that telmisartan has unique properties relative to other ARBs, including potent anti-inflammatory actions and an induction of microglial autophagy, which may enable specific therapeutic uses.
This study aimed to evaluate the efficacy and safety of six ARBs (losartan, valsartan, irbesartan, telmisartan, candesartan, and olmesartan) commonly used to treat hypertension, using a network meta-analysis.
Valsartan and losartan were less effective in lowering blood pressure than other drugs, with no significant differences. Olmesartan and telmisartan were associated with fewer AEs than losartan, although the incidence of adverse events was similar between the other blockers. Olmesartan and telmisartan demonstrated the best balance of antihypertensive efficacy and minimal adverse events. More research is needed to confirm whether telmisartan and olmesartan are optimal choices for controlling blood pressure in patients.
9 Likes
New Aktiia paper by the Aktiia team: Optimizing time-in-target-range assessment for blood pressure: insights from a large-scale study with continual cuffless monitoring
Blood pressure (BP) time-in-target-range (TTR) is an emerging predictor of cardiovascular risk. Conventional BP methods are fundamentally unable to provide an optimal assessment of TTR, using irregular measurements separated by lengthy intervals. We investigated the optimal duration and frequency for reliable, practical TTR assessment in clinical settings using continual monitoring.
This study demonstrated that TTR is markedly impacted by measurement frequency and duration, and that at least one week of 24-h continual monitoring was needed to classify TTR with 90% sensitivity. The contributions of frequency of measurements and duration of measurement were unequal. Even very frequent monitoring over the course of one 24-h period was not sufficient to calculate TTR reliably. Collecting the requisite number and density of measurements is practically achievable only with continual cuffless BP monitors that can generate datasets allowing for TTR classification in real-world clinical use.
Accuracy of ≥90% in TTR classification only occurred with 7 days of continual 24-h monitoring.
2 Likes
My watch notified me of a developing trend in my HRV. For the four years I have measurements on it it, the 30-90-180 day HRV means have been stable at ~46, which is a good but not great value for my age. When I reviewed the dataset, I saw that the upward trend currently in the 60’s corresponds with adding 40 mg. telmisartan to my regimen. I added this ARB to lower my high normal BP into the moderate-low range. As someone whose sympathetic response is above average, there are theoretical reasons why an ARB might increase HRV but I thought it interesting to observe that it might actually be having this effect. I have made no other notable changes in diet, exercise, or lifestyle during this period. The question remains as to whether this HRV increase represents a beneficial change or if it is better characterized as an unmasking of what I have reason to think is good underlying cardiac neurology formerly masked by an overactive sympathetic nervous system.
I’m curious to learn if others have seen changes in their HRV possibly related to ARBs.
4 Likes
Can you say more about these two statements? I wonder if this applies to me too.
As someone whose sympathetic response is above average, there are theoretical reasons why an ARB might increase HRV
How do you know your sympathetic response is above average?
Why do you think an ARB would increase your HRV if you have an above average sympathetic response?
I know a girl who drinks abut a pitcher a day and lowered her BP by 10 points.
I have labile hypertension on telmisartan, but I also had it on lisinopril. I think an amlodipine add-on is more stabilizing, but not at the lower doses.
1 Like
That might lead to too high aluminum and manganese.
A complete answer would require more time than I have before I have to travel @Barnabas. White Coat hypertension can be a common indicator of an exaggerated sympathetic response. There are many others for which, over a lifetime, one observes that their sympathetic system takes over when, objectively, there may be no need.
The theory and research discipline has yet to consolidate but if you Google terms like Telmisartan, HRV, blood pressure, ARBs, stress, sympathetic system, etc. you will uncover an interesting trail of research suggesting that HRV declines when parasympathetic/sympathetic control favors the latter and that stressors (both real physiological and perceived meditated by cognition) are associated with this condition (the actual causal chain can be comp[lex and run in both directions). This is why these two control systems are known as “rest and digest” and “fight or flee.”
If you precede your searches with “SITE: *.GOV” you will mostly retrieve research articles.
2 Likes
Thanks
Still, another cheap intervention to try.
It has higher customer ratings on Amazon, not that it means anything, but most enjoy the tea.
It looks like there are studies to back up the benefits claims. Pub Med has many articles establishing its benefits
"Various review articles have highlighted other potential benefits of hibiscus tea, including:
Several studies have demonstrated the potential of hibiscus tea in lowering blood pressure:
A randomized controlled trial ([2]) found that consuming hibiscus tea for 6 weeks significantly reduced systolic blood pressure (SBP) by 7.2 mmHg compared to placebo in pre- and mildly hypertensive adults.
A systematic review and meta-analysis ([3]) showed a significant reduction in both systolic and diastolic blood pressure with hibiscus supplementation, with greater effects observed in individuals with higher baseline blood pressure levels.
Neuroprotective effects and potential benefits in Alzheimer’s disease ([1])
Nephroprotective, antianemic, antioxidant, anti-inflammatory, and anti-xerostomic activities ([5])
Potential therapeutic applications in cancer and inflammatory diseases ([6])
Antimicrobial and antioxidant activities
Several studies have suggested that hibiscus tea may have beneficial effects on lipid profiles:
A review article ([4]) indicated that hibiscus extracts can improve lipid profiles by reducing total cholesterol, LDL cholesterol, and triglycerides.
A review article ([5]) highlighted the antidyslipidemic effects of hibiscus preparations reported in clinical trials.
1 Like
It seems like a beta-blocker medication (rather than ARB or other BP med classes), especially a B-blocker with low side effects such as nebivolol, would be the ideal antidote for someone with an overly active sympathetic nervous system, since we’re directly targeting receptors for adrenaline/epinephrine. It’s strange to me why there isn’t more research specifically in this area.
2 Likes