Hopefully this week, I’m going to extract the 17-alpha estradiol from the Pantostin. Isopropanol (IPA) and water (two ingredients found in Pantostin) form an azeotropic point, which is difficult to separate using conventional distillation method.
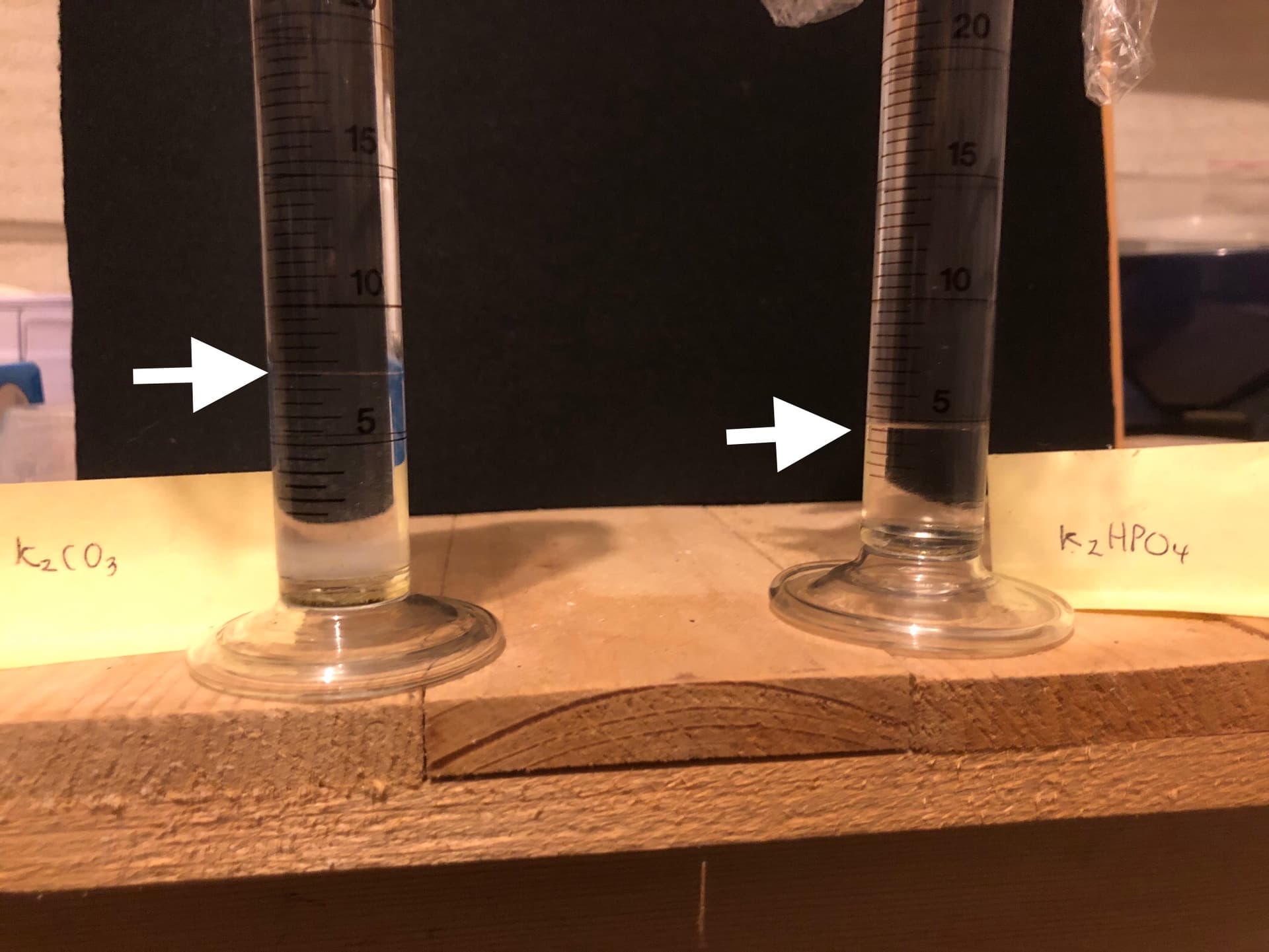
I’m going to use a process called ‘salting out’ where you add a salt to the homogeneous solution, shake, leave it to stand and the water and IPA separates out into two layers. I’ve got two small measuring cylinders and plan to try two salts, potassium carbonate and dipotassium hydrogen phosphate, head-to-head. I think the phosphate salt may be superior in its ability to separate the water from the IPA.
Two hours later - Wow, I was wrong. Seems like carbonate is the way to go, phosphate was hygroscopic and a pain to weight out. Potassium carbonate also salted out a much larger aqueous layer 6.5 mls compared to 3.5mls after compensating for addition of 2g of salt.
Sorry about the quality of the photos it’s very hard to photograph the meniscus.
According to the manufacturer Pantostin, as well as containing IPA and water also contains glycerol and inositol both of which are water soluble and of course 17-alpha estradiol which is water insoluble. So when you ‘salt out’ Pantostin you get an upper layer of IPA which contains 17-alpha estradiol and a lower aqueous layer containing inositol and glycerol.
For the record it seems like Pantostin contains 74% IPA.
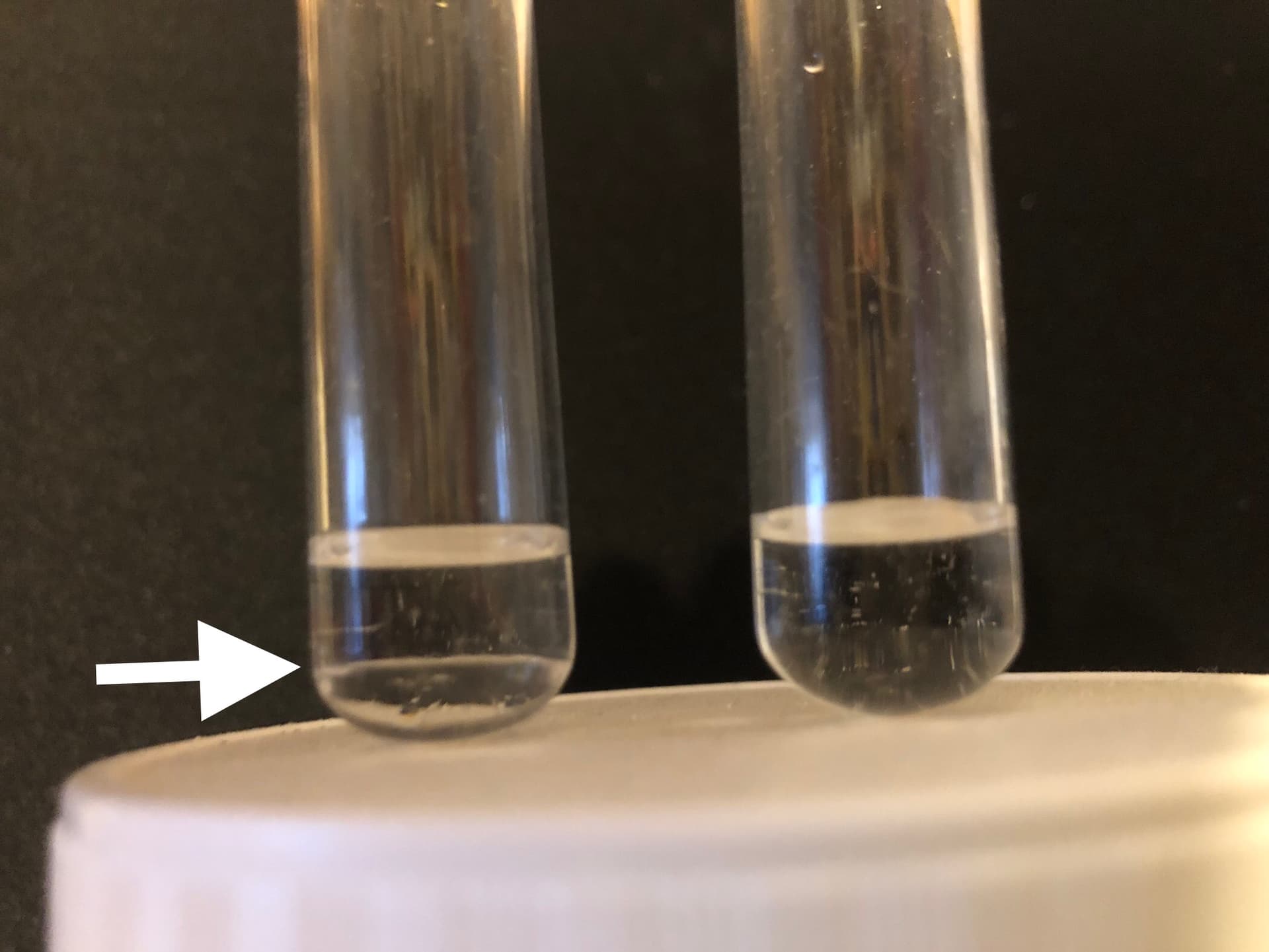
Just to make sure about glycerol I made up two test tubes with glycerol + IPA (left) and glycerol + H2O (right) as you can se below glycerol is immiscible in IPA but soluble in water.
I’m going to leave it overnight, to settle out completely and decant off the organic phase. I’ll then see about doing a second IPA extraction of aqueous layer.
I’m still ‘playing around’ to get an optimal extraction protocol and will post it when I’m happy with it
Great post - thanks for sharing. Please keep us informed on your experiment and explain as much as you can so others can follow and potentially duplicate it.
Many docs and advocates of testosterone replacement therapy (TRT) prefer the sensitive test since it’s more accurate when ensuring that estradiol does not increase to feminizing levels as a response to exogenous testosterone.
Do you guys stop your 17 alpha estradiol application for a couple of days when dosing your weekly rapamycin or do you continue as normal. Would the effects be synergistic to stack 17a with rapa/acarbose ?
I stop the topical application together with all supplements on the days I take Rapa other than Acarbose. Continuing with 17-alpha estradiol may well be synergetic, but it is hard to fully understand how the pathways will impact Rapa. A 24-hour break gives a cleaner opportunity for Rapa to do its magic.
Very interesting experiment! Wanted to check in with you since it’s been 1 year later. Did you end up seeing consistent effects on blood E2 from the Pantostin after upping the dose?
Unfortunately both the Labcorp and Quest tests do NOT detect 17a-E2 reliably but the LC/MS based tests sometimes accidentally reported the 2nd peak that corresponds to 17a-E2 which convinced me that the Pantostin + transcutol (50:50 mix) is actually absorbing the 17a-E2 at around the expected 10% rate. So I continue to take it (expected input of around 50ug/day, from 2ml of Pantostin equal to 4ml of the 50:50 mix) but don’t bother paying extra for the high sensitivity LC/MS based tests.
Thanks for the update! Was it the LC/MS from Labcorp or Quest that you had success with? How high were the reported estradiol numbers that convinced you that it was capturing the 17a-E2 peak?
Of my 2 Labcorp LC/MS/MS tests (see my above post around April 23), one came back “sample error” the other came back after a 17 day delay with a value of 26.1pg/ml for the regular E2 test, and 54pg/mL for the LC/MS/MS version (Labcorp refused to post that result in my patient portal, so I guess I am lucky it got reported at all). The value of 54pg/mL is at the upper end of the range (8-58) for post-menopausal women, corresponding to women on HRT. I was taking 2ml/day of Pantostine, with an expected uptake of 50ug/day (same as my wife’s HRT 17b-E2 patch rated at 50ug/day). I was going to double my intake, but decided against it. I tried to use Quest’s LC/MS/MS E2 test but it just returned the similar value (around 29pg/ml) as their regular E2 test.
I see. That’s promising but wish there was more data. From Half-life of estradiol in postmenopausal women - PubMed a 0.1mg 17b-E2 patch raised levels from 19pg/mL to 112pg/mL. It does seem that getting to steady-state dosing is important prior to measurement as tmax is long (and t1/2 is short).
For the LC/MS, if they saw 2 different peaks, I’d be very surprised if they added the two up instead of just reporting the higher one. Assuming the 54pg/mL only corresponds to the 17a-E2 peak, that would be a high and promising number. Given NIA ITP used a human equivalent of 4.5mg oral (and oral seems to have similar/lower bioavailability vs. transdermal), I do think there’s a lot of upward room for dosing.